Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
Autoimmunity
Rheumatoid Arthritis
Rheumatoid Arthritis
Morgan Alford and Dylan Mann
Learning Objectives
By the end of this section, you will be able to:
Describe the basic anatomy of a synovial joint.
Explain the autoimmune mechanism underlying rheumatoid arthritis.
List extra-articular manifestations of rheumatoid arthritis.
Identify an appropriate therapeutic regimen for a person with advanced rheumatoid arthritis.
Introduction
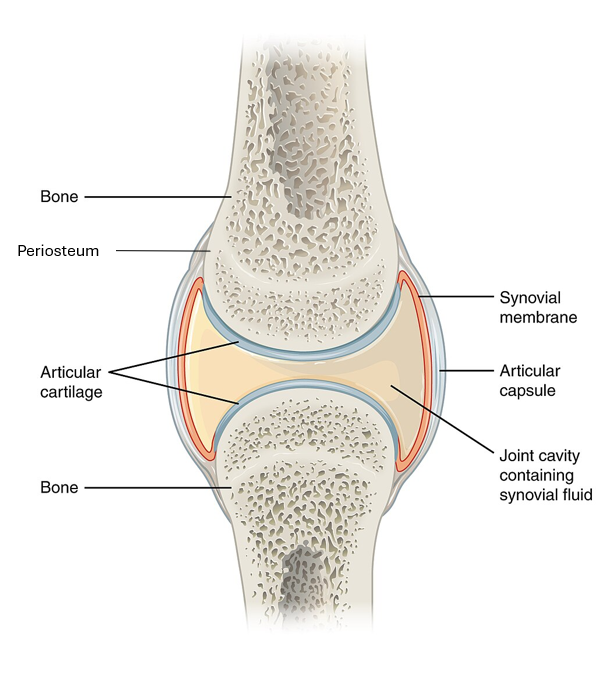
Rheumatoid arthritis is a chronic inflammatory disorder mostly affecting the joints. It is progressive, and can also affect the skin, lungs, and other organ systems. The type of joints that are primarily affected are the synovial joints. Synovial joints include fibrous joint capsules that are continuous with the periosteum . They are also lined with synovial membrane which contains synovial cells that produce lubricating fluid and remove debris. To meet functional and metabolic needs, the synovial membrane has many blood vessels and lymphatics running through them.
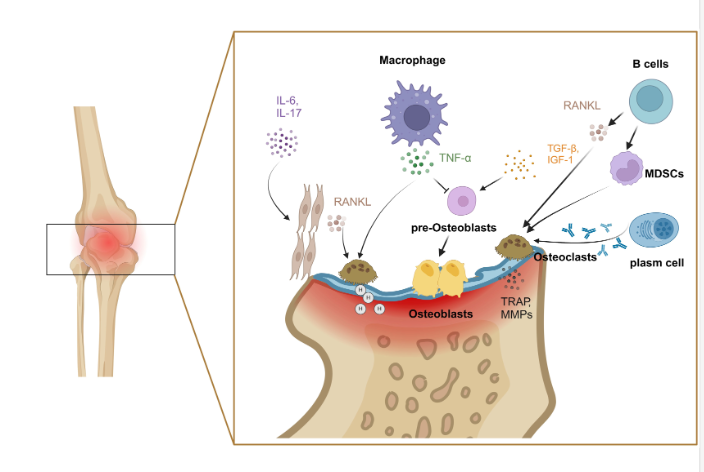
Genetic factors can predispose individuals to developing rheumatoid arthritis, though environmental factors such as infection and exposure to certain chemicals can influence disease pathogenesis. The human leukocyte antigen (HLA) genes that are commonly found in people with rheumatoid arthritis include HLA-DR1 and HLA-DR4. Rheumatoid arthritis can be triggered by modification of type II collagen and vimentin. Type II collagen provides structural support and vimentin influences filament cell migration and deposition in the joint space. Conversion of arginine to citrulline produces modified type II collagen and vimentin which is recognized by immune cells (macrophagesand dendritic cells) as foreign. Then, citrullinated protein antigens are engulfed, processed and presented by antigen-presenting cells that travel to the lymph nodes, where they can activate CD4+ T helper cells. Activated T helper cells may go on to stimulate B cells, which would subsequently differentiate into plasma cells that produce autoantibodies against the self-antigens. Activated T helper cells and antibodies enter circulation and travel to the joints where they may release pro-inflammatory cytokines such as interferon-γ and interleukin-17. Localized macrophages may also contribute to the inflammatory response by producing cytokines such as TNF-α, interleukin-1, and interleukin-6.
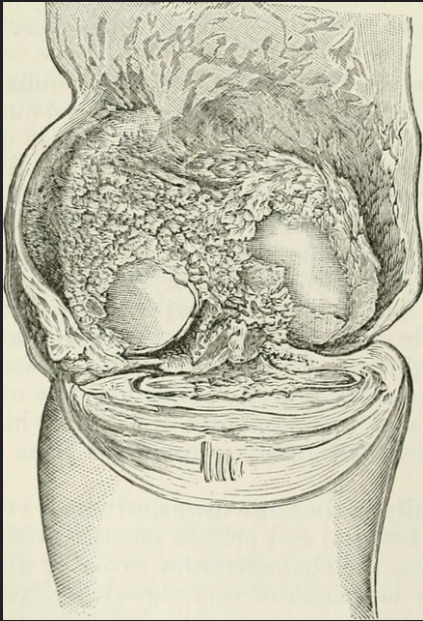
Cytokines raised by immune cells can stimulate synovial cell proliferation in the joints, leading to pannus formation. Over time, the inflamed pannus can damage cartilage and other soft tissues in the joint space since activated synovial cells produce proteases that target articular cartilage. This may cause bony erosions since cartilage loss causes bones to be exposed to each other, which may rub together painfully. Inflammatory cytokines also increase T-cell surface expression of Rank-Ligand , allowing osteoclast activation which would further damage the bones.
Complement Activation Contributes to Disease Progression
As antibodies accumulate in the joint space, a staggering amount of immune complexes form. In the case of rheumatoid arthritis, anti-cyclic citrullinated peptide (anti-CPP) targets citrullinated proteins and forms immune complexes that accumulate in the synovial fluid. Immune complex deposition activates the complement system. The ensuing chronic inflammation causes angiogenesis around the joint, which propagates further inflammation by vascularizing the joint space. Disease progression is characterized by prolonged, extensive inflammation through multiple joints on both sides of the body, which can be destroyed without medical intervention.
Joint Damage
Joints are affected symmetrically, meaning joints on both sides of the body are impacted approximately equally. Initially, rheumatoid arthritis impacts the smaller joints of the hands and feet. These include the metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints of the hand, as well as the metatarsophalangeal (MTP) joints of the feet. Eventually, the disease may spread to large joints such as the shoulders, elbows, knees, and ankles. Flares involve swelling, warmth, redness, and pain in the affected joints. People with rheumatoid arthritis complain of prolonged stiffness after periods of inactivity, especially in the morning. Joint damage may be observed in the hands of people with rheumatoid arthritis patients’ through various signs, including ulnar deviation, buttonhole deformity, extensor tendon splits, hyperextension, and swan neck deformity. Identification of these deformities is important in aiding medical professionals’ treatment and monitoring of disease progression.
Inflammatory cytokines can have long-ranging extra-articular impacts on the body. These signaling molecules can travel via the circulatory system to wreak havoc in multiple organ systems. For example, Interleukin-1 and interleukin-6 can cross the blood-brain barrier and induce fever. In the skin, rheumatoid nodules arise from granuloma formation. In blood vessels, inflammation promotes deposition of atheromatous plaques, increasing an individual’s risk of heart attack. In the liver, hepcidin may sequester iron and lead to anemia. In the lungs, activated fibroblasts may contribute to formation of scar tissue, making gas exchange more difficult. The pleural cavity may also fill with fluid, which would decrease lung capacity. It is important to acknowledge that RA symptoms are not limited to the joints, and thus crucial to consider when treating and monitoring the disease.
Diagnosis and Treatment
Clinicians will test for rheumatic diseases when patients present with symptomology consistent with the clinical picture of rheumatoid arthritis. Clinicians may test for rheumatoid factor and anti-citrullinated peptide (anti-CCP) antibody titres. While rheumatoid factor remains a useful biomarker, anti-CCP reliably differentiates rheumatoid arthritis from other rheumatic diseases. Another important diagnostic tool is X-ray imaging, which may reveal decreased bone density around affected joints, soft tissue swelling, narrowing of the joint space, and bony erosions.
Long-term treatments for RA are classified as follows. Disease modifying anti-rheumatic medications (DMARDs) include the drugs methotrexate, hydroxychloroquine and sulfasalazine, which are anti-inflammatory therapeutic agents. Biologics, which act to block or suppress specific proteins or cells, include abatacept (T cell suppressor), Rituximab (B cell suppressor), and others that block chemokines, immunoglobulins and interleukins. Acute flares can be treated using non-steroidal anti-inflammatory agents (NSAIDs) and glucocorticoids. NSAIDs include over the counter drugs such as Ibuprofen and aspirin, which act by blocking enzymes that elicit pain and inflammation. Glucocorticoids similarly act by blocking production of inflammatory cells, however, are typically more potent then NSAIDs and require prescription.
Dense layer of connective tissue enclosing the bones except at the surface of joints
genes part of the major histocompatibility complex
large phagocytic cell that engulfs foreign particles and pathogens
immune cell that processes antigen material and presents it on the surface of other cells to induce an immune response
immune cell that detects, engulfs, and informs the adaptive immune response about an infection by presenting the processed antigen on the cell surface
abnormal layer of fibrous and granular tissue, often formed in the joints, cornea, or heart valves
Protein involved in bone metabolism, and key regulator of osteoclast formation, activation, and survival
array of approximately 20 soluble proteins of the innate immune system that enhance phagocytosis, bore holes in pathogens, and recruit lymphocytes; enhances the adaptive response when antibodies are produced
process in which new blood vessels form from existing ones
pockets of infected tissue walled off and surrounded by white blood cells



{kind=link}
{kind=link}
{kind=link}