Autoimmunity
Graves’ Disease
Graves' Disease
Dylan Mann and Morgan Alford
Learning Objectives
By the end of this section, you will be able to:
- Describe normal thyroid function and anatomy, highlighting key hormones and processes.
- Outline the autoimmune mechanism behind Graves disease incidence.
- Describe symptoms, treatment, and diagnosis of Graves disease.
Introduction
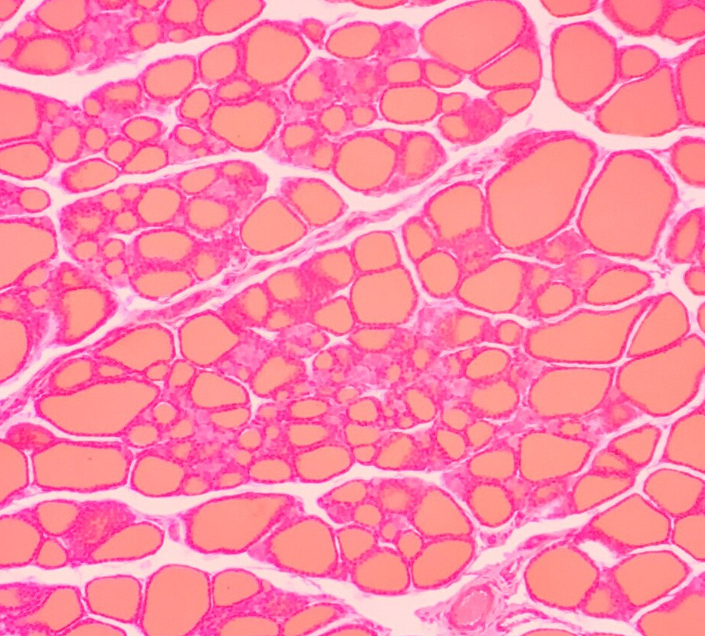
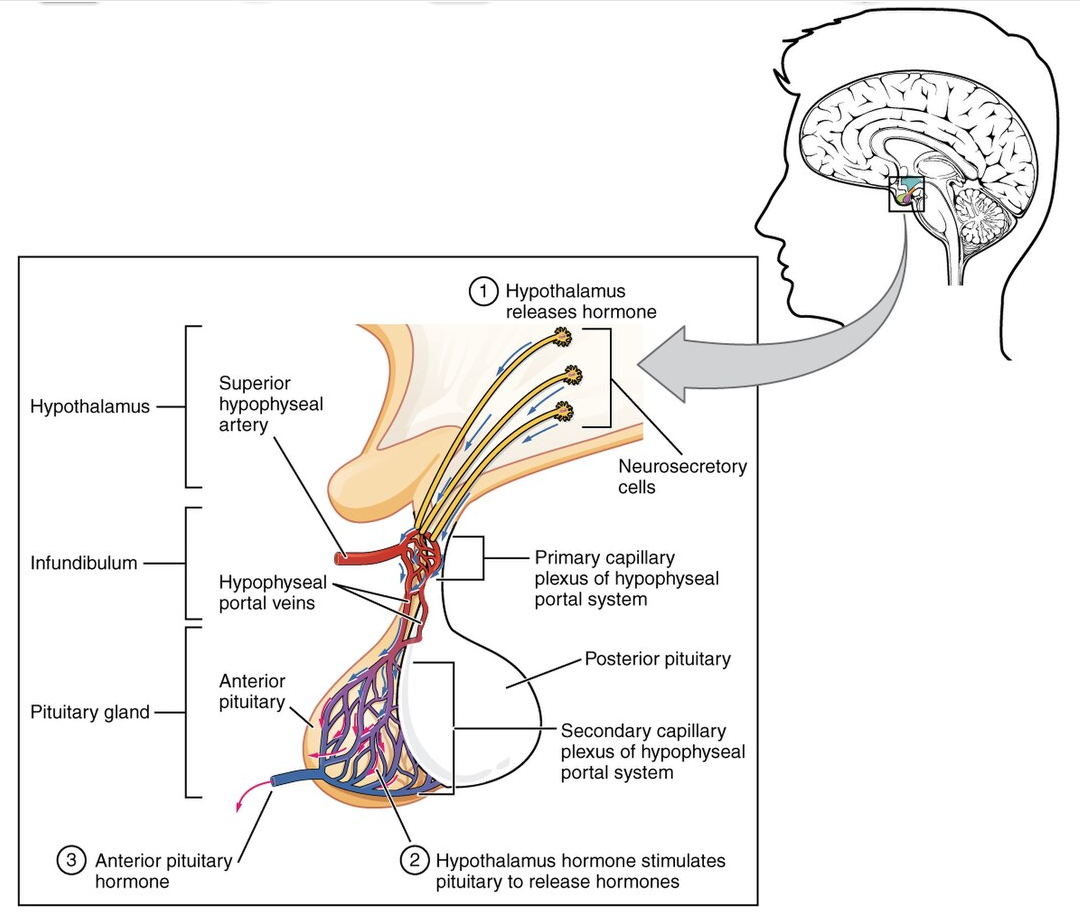
Normal Thyroid Function and Anatomy
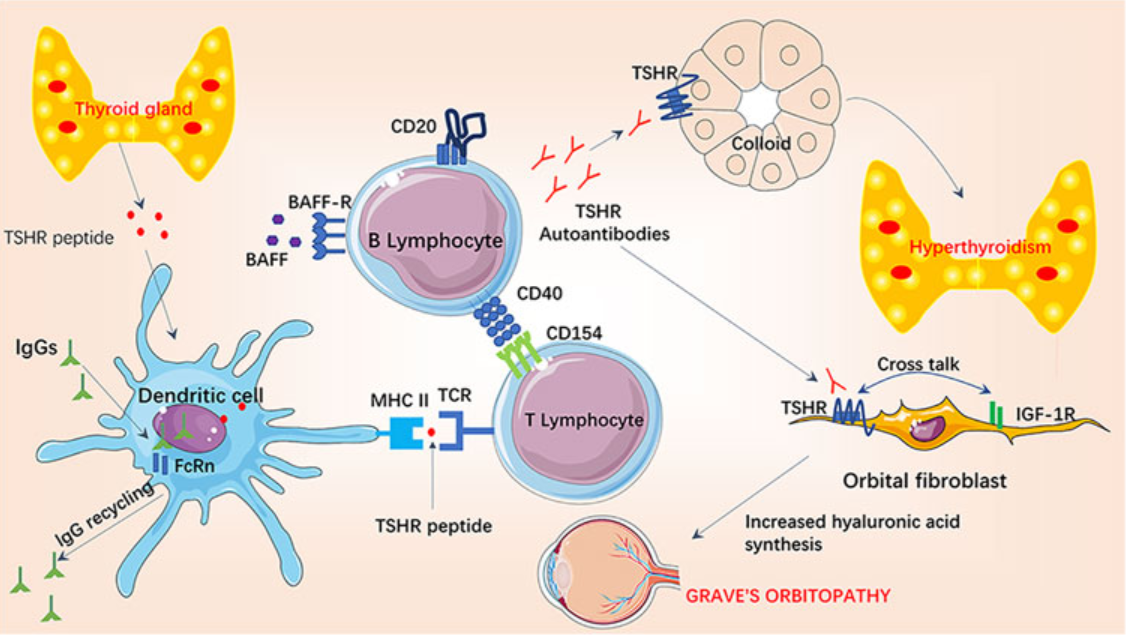
Autoimmune Mechanism
Symptoms
The main symptoms of Graves’ disease include hyperthyroidism, ophthalmopathy, and dermopathy.
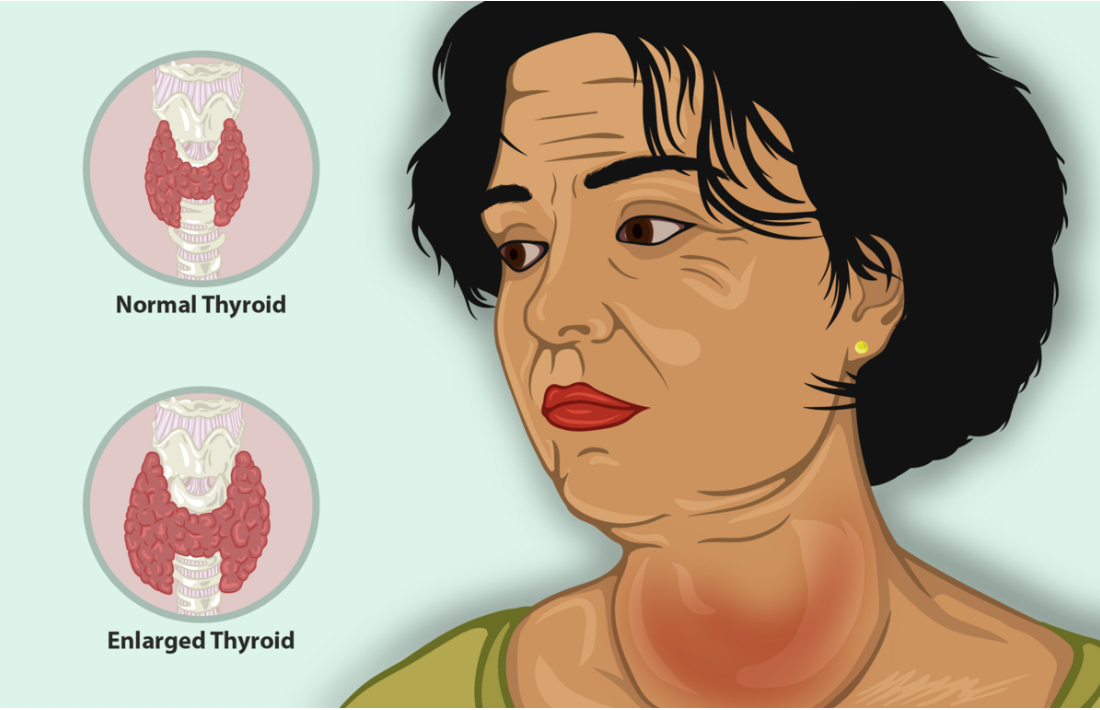
Untreated hyperthyroidism can lead to significant weight loss despite increased appetite due to increased basal metabolic rate, which coincides with overall heat intolerance. Hyperthyroidism also causes an increase in sympathetic nervous system activity, which may cause rapid heart rate, sweating, hyperactivity, anxiety, and insomnia. As described above, hyperthyroidism may also lead to a goiter, characterized by hyperplasia and hypertrophy of the thyroid tissue.
In Graves ophthalmopathy, a buildup of glycosaminoglycans causes inflammation and swelling in and around the eye’s follicular cells. This process can lead to exophthalmos, which is an outward bulging of the eyeball. Furthermore, this weakens the muscles that control upper eyelid movement and may damage the cornea as the individual has a difficult time blinking efficiently. Together, Graves ophthalmopathy symptoms lead to an increased risk of corneal ulcers.

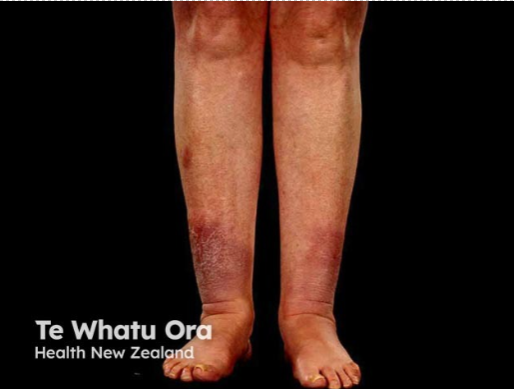
Graves dermopathy is characterized by localized thickening and swelling of the skin due to glycosaminoglycan build-up. This is a rare skin condition marked by non-pitting edema, particularly over the shins.
People with Graves’ disease can experience an acute flair in their disease called a ‘thyroid storm’. A thyroid storm is a life-threatening increase in hyperthyroidism where the body goes into a state of sever hypermetabolism. A flare such as this can develop when a patient stops their treatment, develops infection, or has surgery. During a thyroid storm, all normal symptoms of hyperthyroidism become exaggerated. For example, heat intolerance can develop into high fever and a rapid heart rate can develop into cardiac arrythmia.
Diagnosis and Treatment
Diagnosis of hyperthyroidism is done through blood tests, where levels of TSH, T3, and T4 are measured. To confirm if hyperthyroidism is caused by Graves’ disease, a blood test measuring thyroid stimulating antibodies would be performed. To further support diagnosis, radioiodine scans and measurements of iodine uptake would subsequently be tested. Radioiodine scans work by injecting small amounts of radioactive iodine, which can be traced endogenously through advanced cameras. Imaging allows medical professionals to monitor iodine absorption and function of the thyroid.
The main treatment approach for Graves’ disease includes medication. Beta blockers treat the immediate symptoms of hyperthyroidism. Beta blockers do not act by directly reducing thyroid hormone production; instead, they block beta-adrenergic receptors. These receptors are the site of induction of sympathetic nervous system activity. Therefor the use of beta-blockers causes a reduction in the sympathetic nervous system hormones epinephrine and norepinephrine. Specific beta blockers may also help reduce or block the conversion of T4 into the more potent thyroid hormone T3. Anti-thyroid drugs however may directly block thyroid hormone production and release. In severe cases, the thyroid may need to be destroyed or removed. Radio-iodine therapy partially destroys thyroid function but requires subsequent hormone replacement therapy. If the goiter becomes so large that it presses against surrounding tissue, thyroid tissue can be removed through surgery. Graves ophthalmopathy is treated separately, using steroids, radiation therapy, and surgery. Graves dermopathy is generally treated through overall stabilization of the disease, however topical immunosuppressant may be used to specifically reduce the autoimmune response in affected areas.
Review Questions
Media Attributions
- Thyroid follicle section under light microscope © Panzer is licensed under a CC BY-SA (Attribution ShareAlike) license
- The hypophyseal portal vein connects the hypothalamus to the anterior pituitary © OpenStax College is licensed under a CC BY (Attribution) license
- Graves disease autoimmune mechanism, including important players leading to hyperthyroidism © He et al. is licensed under a CC BY (Attribution) license
- Thyroid enlargement, a symptom of hyperthyroidism can result in a structure called a Goiter is licensed under a CC BY-SA (Attribution ShareAlike) license
- Graves’ disease induced ophthalmopathy © Sim Peini is licensed under a CC BY (Attribution) license
- Graves induced dermopathy, most commonly resulting in non pitting edema on the shins © Gardner et al. is licensed under a CC BY-ND (Attribution NoDerivatives) license
hormone produced in the hypothalamus that stimulates the release of thyroid-stimulating hormone in the anterior pituitary gland
hormone produced by the anterior pituitary gland that stimulates the thyroid gland to produce thyroid hormones
thyroid hormone that has many regulating effects in the body such as metabolism, growth, body temperature, and heart rate.
primary hormone produced by the thyroid gland. Is the pro hormone form of the more active form thyroid hormone triiodothyronine.
type of hypersensitivity reaction in which antibodies bind to antigens on the surface of cells or extracellular materials, triggering an immune response that damages or destroys those cells or tissues
lymphocytes that mature in the bone marrow and differentiate into antibody-secreting plasma cells
protein that is produced by plasma cells after stimulation by an antigen; also known as an immunoglobulin
Proteins produced by the immune system which recognize and neutralize antigens. Also known as antibodies
tissue is enlarged due to each individual cell becoming larger, often with an increase of cytoplasmic contents such as contractile proteins as in the case with muscle tissue
An enlargement of a tissue or organ caused by an abnormal increase in the number of cells in a tissue or organ
Cell type found in connective tissue, responsible for producing and maintaining the extracellular matrix
occurs when the thyroid gland releases excessive amounts of thyroid hormones into the bloodstream. Can lead to dramatic increase in hyperthyroidism and its symptoms.

{kind=link}
{kind=link}
{kind=link}