Autoimmunity
Systemic Lupus Erythematosus
Systemic Lupus Erythematosus
Dylan Mann and Morgan Alford
Learning Objectives
By the end of this section, you will be able to:
- Describe the autoimmune reaction behind Systemic Lupus erythematosus development.
- Explain how sex hormones lead to unequal incidence rate among biological males and females.
- Overview System Lupus erythematosus diagnosis, treatment, and symptoms.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune condition that can affect many organs and tissues, including the skin. SLE may develop in a person who carries some combination of susceptibility genes and is exposed to an environmental trigger. Susceptibility genes, much like other autoimmune conditions discussed in this chapter, are most commonly found in the human leukocyte antigens (HLA), which present antigens to T cells.
Manifestation of Autoimmune Reaction
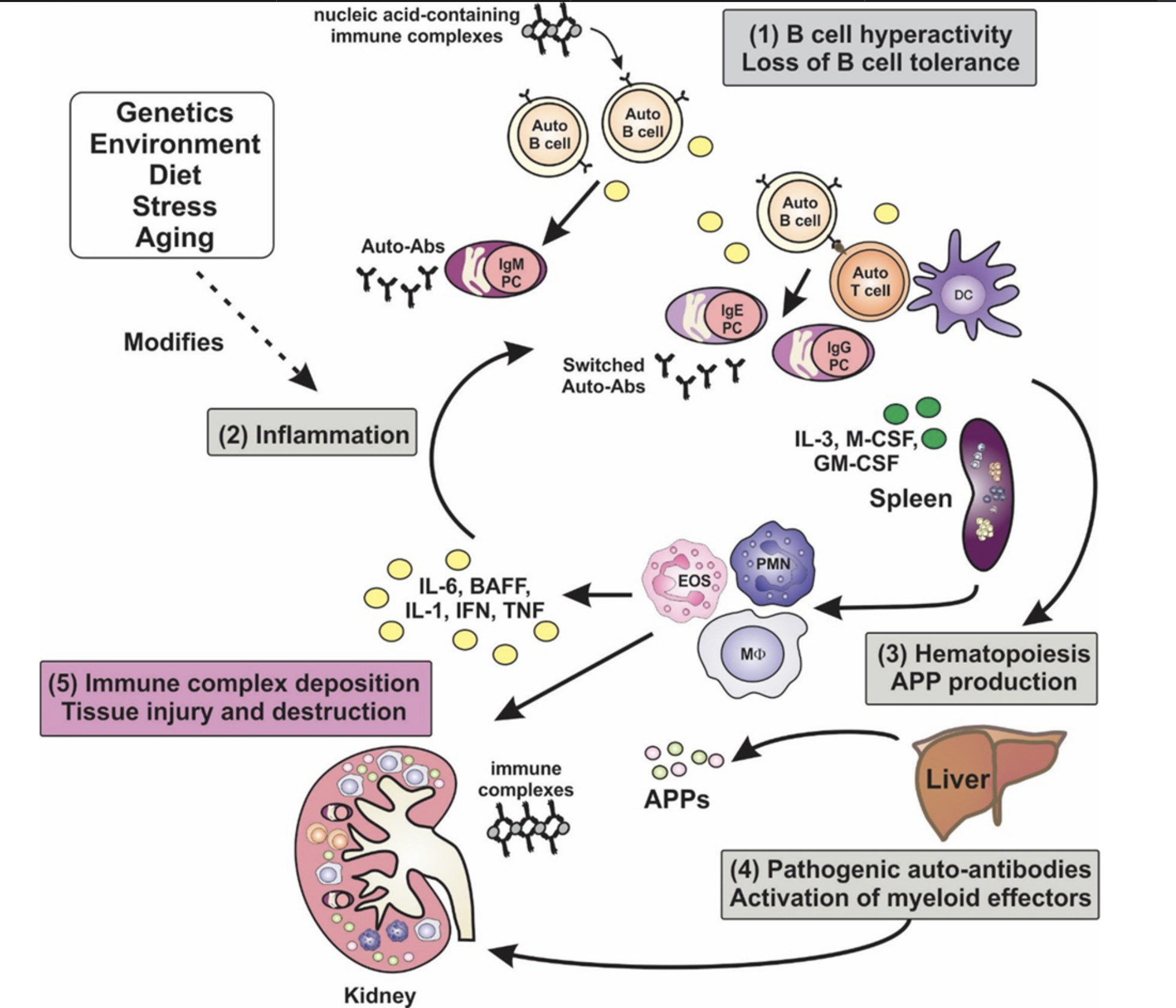
SLE can be triggered by DNA damage. Environmental triggers include but are not limited to sunlight (UV radiation), inhaled smoke, bacteria, viruses, and medication. When DNA is damaged, the cell may repair the damage or undergo programmed cell death, in which apoptotic bodiescontaining DNA, histones, and other nuclear proteins are released from the cell. Apoptotic bodies containing nuclear antigens may stimulate an auto-immune process. Since susceptible individuals demonstrate reduced clearance of nuclear antigens, B cells may begin producing anti-nuclear antibodies (ANAs) to neutralize the attack.
Complement System Leads to Type III Hypersensitivity Reaction
ANAs will bind to nuclear antigens with a high degree of specificity. The resulting complexes will travel to many different tissues via the circulatory system, where they may deposit (particularly at ultrafiltration sites). The most common sites of deposition are in the skin, kidney, heart and joints. Complex deposition may initiate localized inflammation and complement system activation, which may lead to increased cell damage and apoptosis, promoting release of nuclear antigens further. Since the inflammatory cascade was stimulated by immune complex deposition, it is a prime example of a type III hypersensitivity reaction.
Sex Hormones Cause an Unequal Incidence Rate among Biological Males and Females
Estrogen plays an important role in the incidence of SLE. Estrogen levels are positively correlated to white blood cell count and robustness of immune activation. Women of child-rearing age (when peak estrogen levels are observed) are diagnosed with SLE 10x more frequently than men. However, older or younger women are diagnosed with SLE only 2x more frequently than men.
SLE Antibody and Antigen Development is not Limited to Nuclear Components
People living with SLE develop antibodies targeting both nuclear and non-nuclear antigens. For example, patients can acquire blood auto antibodies that may lead to hematologic disorders such as anemia, cytopenia, or leukopenia. Anti-smith antibodies target nuclear components such as ribonucleoproteins, and anti-dsDNA target double stranded DNA found in nuclei and are both specific to SLE. Another type of antibody includes anti-phospholipid antibodies, which usually target protein bound to phospholipids. Antibodies targeting phospholipids are particularly problematic, as phospholipids are found in cell membranes across all tissues. Such antibodies can lead to anti-phospholipid syndrome, where antibodies cause a hypercoagulable state. This causes the patient to be more prone to clots, deep vein thrombosis, hepatic vein thrombosis, and stroke.
Diagnoses and Symptoms
Given the systemic nature of SLE, symptomology is highly variable, which presents diagnostic challenges. General symptoms may include fever and weight loss, but specific symptoms depend on the affected tissues. Diagnostic criteria can be classified by the inflicted system: skin, mucosa, serosa, kidneys, joints, brain, blood, and immunity (antibodies).
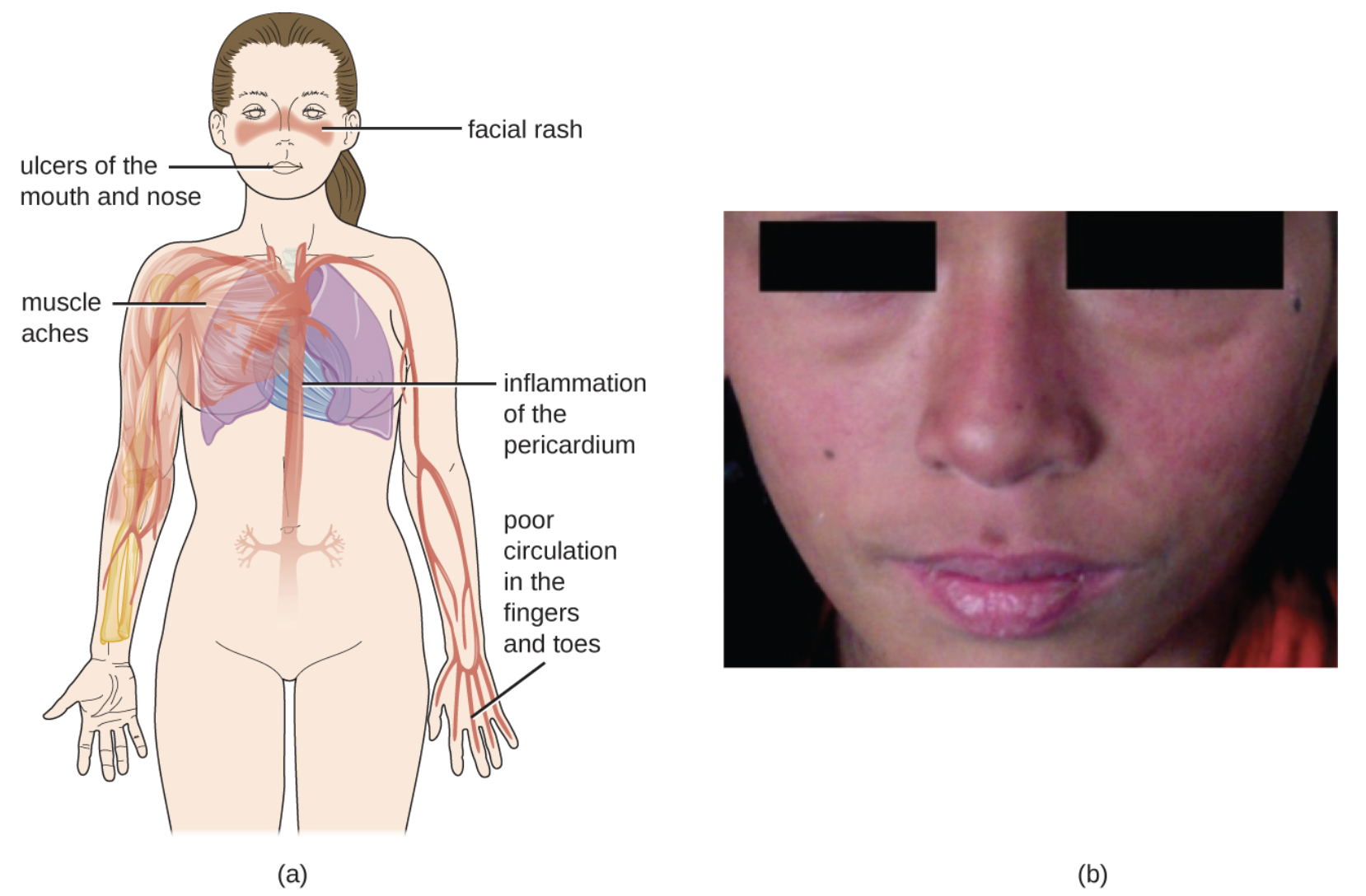
Symptoms observed in the skin may include the malar (butterfly) rash, discoid rash, and photosensitivity. People with SLE infrequently report ulcers of the mucosa. Serosal inflammation may present as pleuritis, pericarditis, or endocarditis. Patients often experience joint pain and inflammation (arthritis) which can lead to permanent damage if left untreated. Additionally, individuals may exhibit proteinuria or glomerulonephritis. Severe neurological symptoms include seizure, whereas hematological symptoms include decreased counts of red and/or white blood cells. Most people living with SLE will test positive for ANAs, though the test is not specific enough to be used on its own.
Clinicians seek to identify at least four of the 11 diagnostic criteria in a patient before making a diagnosis of SLE and initiating a person on treatment to manage flare ups.
Treatment
People with SLE alternate between states of flare and remittance. Immunosuppressant drugs, which may limit the autoimmune response topically or systematically, may be used to control flare ups. During periods of remittance, it is advised to avoid triggers including sunlight (UV) exposure and smoke in addition to practicing good hygiene.
Review Questions
Media Attributions
- Figure highlighting key cells, tissues, and processes in autoimmune development of Systemic Lupus Erythematosus © Gottschalk et al. is licensed under a CC BY (Attribution) license
- Figure highlighting common SLE symptoms, upclose image on the right shows development of a malar rash. © CNX OpenStax is licensed under a CC BY (Attribution) license
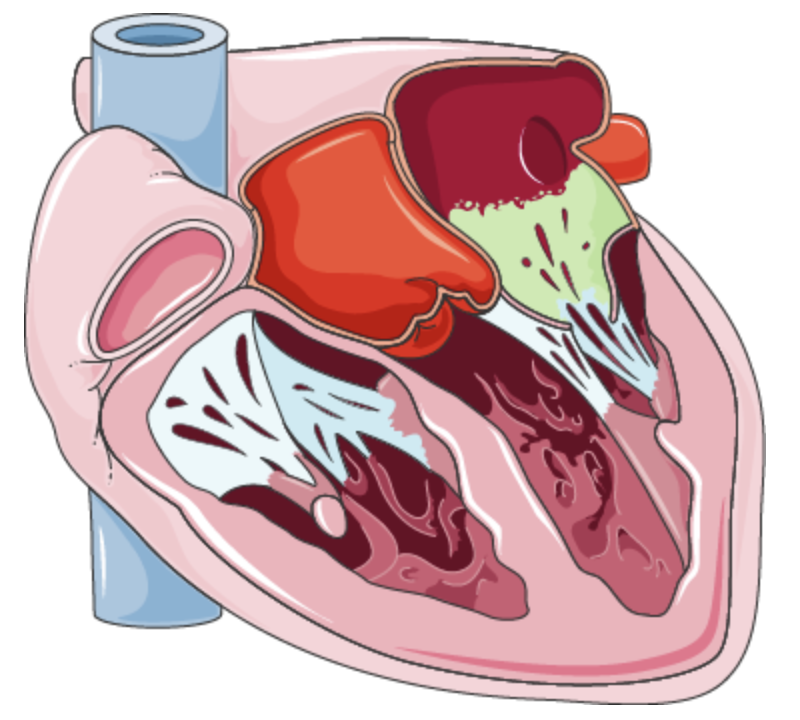
- The most common cardiac manifestation of SLE includes Libman Sacks Endocarditis. This is a form of non bacterial endocarditis in which the inner layer of the heart become inflamed. © Content Partnerships Hub is licensed under a CC BY-SA (Attribution ShareAlike) license
Autoimmune disease in which the immune system mistakenly attacks a wide variety of organs and tissues.
small membrane-bound vesicles released from cells undergoing apoptosis
Antibody that the immune system makes to mistakenly attack the nucleus of its own cells
array of approximately 20 soluble proteins of the innate immune system that enhance phagocytosis, bore holes in pathogens, and recruit lymphocytes; enhances the adaptive response when antibodies are produced
Immune reaction where circulating antigen-antibody complexes deposit in tissues, leading to inflammation and tissue damage

{kind=link}
{kind=link}