Neuromuscular Control of Motion
Pathophysiology of Neuromuscular Control: Issues with Neuromuscular Junction (Myasthenia Gravis)
Valerie Swanston and Carter Allen
Learning Objectives
By the end of this section, you will be able to:
- Define Myasthenia Gravis.
- Explain the pathophysiology of Myasthenia Gravis.
- Identify the common signs and symptoms seen in Myasthenia Gravis.
- List treatments for Myasthenia Gravis.
Recall what we learned about the NMJ. An action potential is conducted down a motor neuron and travels to the axon terminal, triggering the opening of Ca2+ channels. Influx of Ca2+ ions into the neuron causes V-snare proteins on the vesicles to bind with T-snares on the synaptic bulb membrane leading to release of the neurotransmitter acetylcholine (ACh). In the synaptic cleft, ACh binds to ACh receptors (AChR) on the muscle fibre end plate, triggering a new action potential in the sarcolemma of the muscle fibre (end plate potential). The action potential leads to a conformational change in certain receptors (also along the sarcolemma) which opens flow of Ca2+ out of the sarcoplasmic reticulum (which is where calcium is stored in muscles). Ca2+ binds to troponin which causes a conformational change, exposing the actin to myosin heads, which leads to cross bridging, which causes contraction of the muscle.
Pathophysiology of Myasthenia Gravis
Myasthenia Gravis (MG) is an autoimmune disorder, meaning it is caused by the body’s immune system mistakenly identifying normal parts of the body as foreign and mounting an immune response against them. The identification of self peptides as foreign by helper T-cells leads to B-cells production of autoantibodies (antibodies against self) to a variety of proteins involving ACh transmission at the neuromuscular junction (NMJ). This interrupts acetylcholine action at the NMJ, preventing the neural control of voluntary motor movement. The following are the kinds of autoantibodies associated with Myasthenia Gravis.
1: Anti AChR Autoantibodies
This is the most common presentation of MG and most MG patients with autoantibodies against other proteins will also test positive for AChR autoantibodies. The AChR autoantibodies are thought to block transmission through the NMJ by three mechanisms:
- Autoantibodies competitively antagonize AChR therefore inhibiting ACh binding.
- Promoting endocytosis (internalization) of AChR into the muscle fibre so it is no longer at the cell surface.
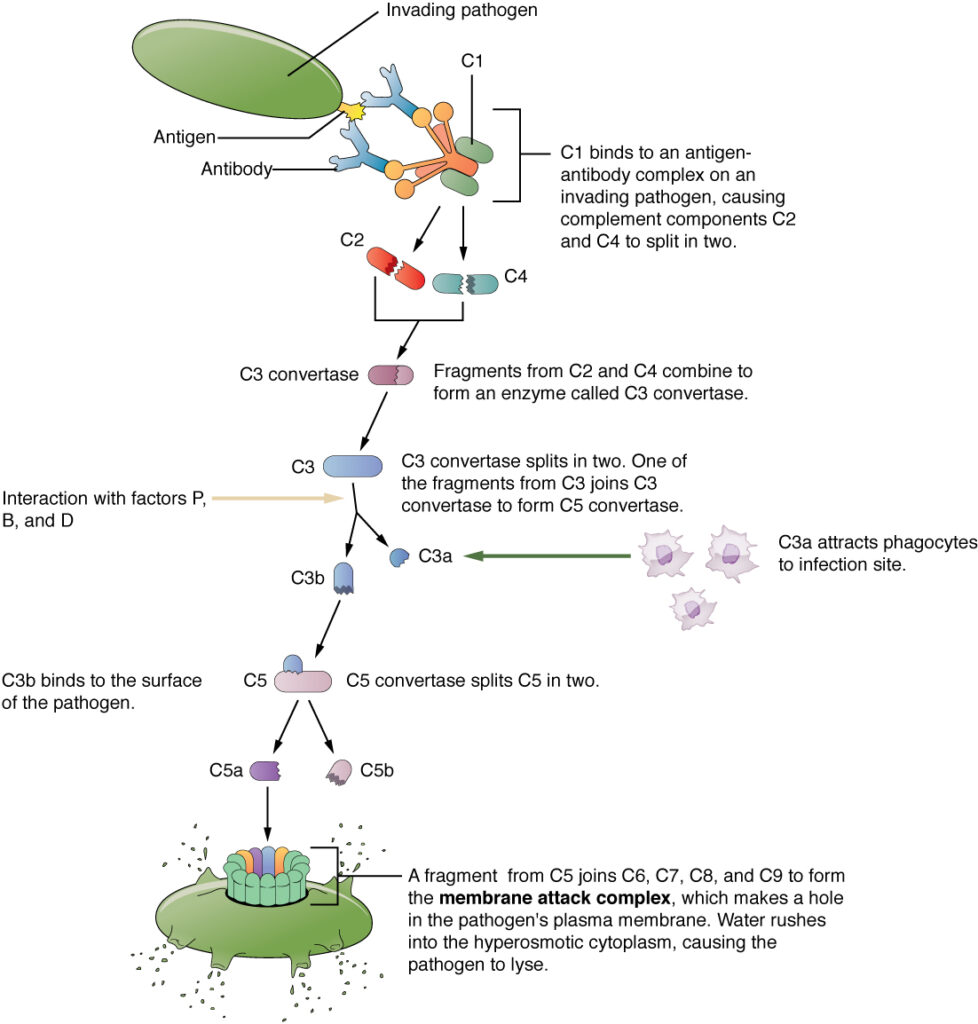
- Activate complement. The complement cascade outlined below will inevitably lead to the creation of the membrane attack complex, which will bring about the lysis of the postsynaptic membrane.
2: MuSK Autoantibodies
MuSK is a protein expressed only in our skeletal muscle, it is thought to play a key role in presentation of high density of AChR at the NMJ. Thus antibodies against MuSK will result in less receptors on the muscle to start initiation of contraction.
3: LRP-4 Autoantibodies
LRP-4 acts upstream in regulation of AChR clustering much like MuSK, and regulation of presynaptic membrane organization. [1]
4: Agrin Autoantibodies
Agrin is a protein responsible for the activation of MuSK.
5: Cortactin Autoantibodies
Cortactin is involved in regulation of both synaptic and post synaptic membranes at the NMJ. [2]
As a result of inhibition destruction of any of these structures by autoantibodies, communication between the muscle and motor neuron is blocked or impaired, leading to fluctuating muscle weakness.
Clinical Presentation
MG appears more frequently either before the age of 30 or at 50 yrs and older. MG has a higher frequency in females less than 30 years of age, which is typical of autoimmune disorders. Patients with MG most commonly present with symptoms involving the fatiguing of ocular muscles. This often presents as ptosis, a characteristic “drooping” of the eyelid.
There are two kinds of MG: ocular (localized in eye muscles) and generalized. As mentioned, patients most often present with only eye symptoms. Ocular MG presents with signs and symptoms isolated only to the eye(s) and vision. Ocular MG presents with ptosis, decreased movement of the eyeball, and weakness of the eyelids. Ocular MG can progress to generalized MG. Patients with generalized MG may also have ocular symptoms.
Patients with MG often have muscle weakness that gets worse throughout the day. When disease spreads to different muscle groups it can cause a host of different problems including trouble regulating swallowing (dysphagia), trouble speaking (dysarthria), and reduced facial expression. Patients’ dysphagia might cause them to need to be put on special diets. Patients may reduce their oral intake because of fatigue of chewing and swallowing muscles. In the appendages patients will have muscle weakness. This generally affects proximal muscles (closer to the torso) more than distal ones. In extreme cases, severe weakness of respiratory muscles can cause respiratory failure requiring mechanical ventilation.
Did you know: botulinum toxin
You may have heard of people getting “Botox” treatments for cosmetic reasons, such as reducing the appearance of facial wrinkles. The substance responsible for this effect is botulinum, a neurotoxin produced from the bacteria Clostridium botulinum. Similarly to the AChR autoantibodies in MG, botulinum acts at the NMJ to prevent transmission of action potentials from the motor neuron to the muscle fibre. However, its exact mechanism is different; it acts at the axon terminal at the motor neuron by preventing ACh release. Botulinum is injected into the facial muscles to force them to relax, which has a smoothing effect on the overlying skin. Botulinum is also used for medical reasons such as treating muscle spasticity.
Diagnostic Tests
To determine whether ocular symptoms are caused by MG vs other neuromuscular pathologies, a series of clinical exams for fatigue of eye muscles during gaze and unsynchronized eyelid movements.
In addition to clinical presentation, diagnosis can be made by investigating the presence of autoantibodies to AchR. A serum sample is taken and tested for Myasthenia Gravis antibodies.[3]
Treatment of MG
Acetylcholinesterase breaks acetylcholine down into acetate and choline in the synaptic cleft of an NMJ. Therefore inhibition of acetylcholinesterase will lead to an increase of acetylcholine available in the NMJ, which will compensate for a reduction in the number of active receptors
Immunosuppressants inhibit the production and release of interleukin II which reduces proliferation and activity of T-cells and B-cells (which produce antibodies)
Corticosteroids suppress the immune and inflammatory response. Immunosuppressant medications that reduce the expression and activity of immune cells in the body.
Complement Interruption
Drugs that act as antibodies which can block or even signal for the destruction of complement proteins. Blocking the correct complement proteins, such as C5, can effectively stop the complement cascade.[5]
Thymectomy
Removal of the thymus gland can reduce autoimmunity, as the thymus is where T-cells mature.
Plasmapheresis
Machine filtration of autoantibodies out of blood. This however does not prevent the production of new autoantibodies, and is therefore only a temporary treatment
Intravenous Immunoglobulin
Influx of detectable antibodies in the body reduces the production of autoantibodies.[6]
Review Questions
Media Attributions
- 2212_Complement_Cascade_and_Function © OpenStax College is licensed under a CC BY (Attribution) license
- https://www.ncbi.nlm.nih.gov/gene/228357 ↵
- Alicea, D., Perez, M., Maldonado, C., Dominicci-Cotto, C., & Marie, B. (2017). Cortactin is a regulator of activity-dependent synaptic plasticity controlled by wingless. The Journal of Neuroscience : The Official Journal of the Society for Neuroscience, 37(8), 2203–2215. https://doi.org/10.1523/JNEUROSCI.1375-16.2017 ↵
- National Institute of Neurological Disorders and Stroke. (2024). Myasthenia gravis. www.ninds.nih.gov. https://www.ninds.nih.gov/health-information/disorders/myasthenia-gravis ↵
- http://online.lexi.com.eu1.proxy.openathens.net/lco/action/search?q=myasthenia%20gravis&t=name&acs=true&acq=mysthe ↵
- http://online.lexi.com.eu1.proxy.openathens.net/lco/action/doc/retrieve/docid/patch_f/810198?cesid=2hfu8d4vGPX&searchUrl=%2Flco%2Faction%2Fsearch%3Fq%3Deculizumab%26t%3Dname%26acs%3Dfalse%26acq%3Deculizumab# ↵
- National Institute of Neurological Disorders and Stroke. (2024). Myasthenia gravis. www.ninds.nih.gov. https://www.ninds.nih.gov/health-information/disorders/myasthenia-gravis ↵

{kind=link}