Neuromuscular Control of Motion
Clinical Manifestations of Neuromuscular Disorders
Valerie Swanston
Learning Objectives
- Describe the clinical manifestations of traumatic brain injury, ischemic stroke, multiple sclerosis, and peripheral neuropathies
Now that we have learned about multiple different conditions affecting the neuromuscular system, let’s put this information together to understand how there can be many possible etiologies (causes) of a patient experiencing a neuromuscular symptom or deficit. Starting from top to bottom, muscle contraction is initiated in the motor association areas and primary motor cortex in the frontal lobe of the cerebral cortex. An action potential is transmitted down the upper motor neuron through the brainstem and spinal cord, which synapses with a lower motor neuron in the anterior horn of the spinal cord. The lower motor neuron exits the spinal cord in the anterior root and travels to the muscle. Action potential transmission at the synapse between the lower motor neuron and the muscle fibre (also known as the NMJ) results in contraction of the muscle and production of voluntary movement. Weakness or paralysis of a muscle may be due to interruption at any point along this pathway. Think about the pathophysiology of the neuromuscular conditions we just learned about and how they may interrupt this pathway and result in motor symptoms, as demonstrated the figure below.
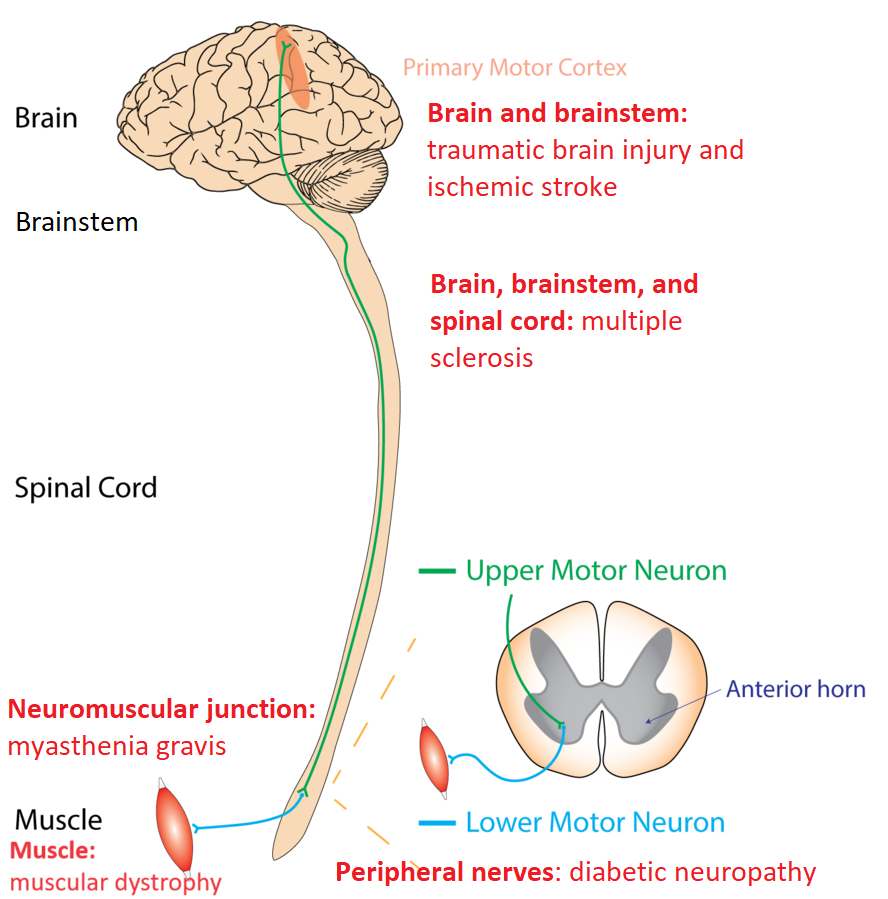
In this chapter, we will discuss some of the typical neuromuscular deficits observed in each condition we learned about previously. Think back to the pathophysiology of each condition and see if you can rationalize the symptoms we’re learning about.
Direct Observations of Neuromuscular Disorders
Patients realize they have a neuromuscular disorder before any test is taken: mostly because it is affecting their activities of daily living. However, problems with voluntary movement is a manifestation of impairments of the incoming sensory message, outgoing motor message, the neuromuscular junction, or muscle contraction. By observing the following changes, one can hone in on the site of pathology.
While the clinical examination of neuromuscular disorders is out of the scope of this book, there is another Open Education resource which demonstrates these clinical examinations. Clinical neurological exams. A skilled health care practitioner will be able to determine normal vs. impaired neuromuscular functions and whether these impairments are on the sensory, motor, or both sets of nerves. These test results are loosely summarized as below.
| Clinical Manifestation | Impairment of sensory, motor, or both |
| Changes in sensation in a localized area | Ascending sensory nerve, spinal cord (sensory), brain |
| Changes in sensation in different geographic locations | Ascending sensory nerve, spinal cord (sensory), brain |
| Decrease in sensation AND motor in the same localized area | Peripheral nervous system (esp where sensory and motor nerves are bundled together) |
| Changes in speed or strength of motor movement | Descending motor nerve (upper/lower motor neuron), neuromuscular junction |
| Changes in muscle bulk | Loss of muscle tissue or loss of muscle tone due to decr nervous control |
| Changes in reflex | Spinal cord at the level of the reflex, lower motor neuron, |
| Loss of sensation and motor | Brain |
| Changes in motor in different geographic locations | Upper/lower motor neuron; peripheral nervous system? |
Clinical manifestations and where the area of impairment lies
Traumatic Brain Injury
A traumatic brain injury (TBI) can have a severe impact on the health and function of the brain, brainstem, and/or spinal cord. Many TBI patients experience significant neuromotor dysfunction and disability, at times for the rest of their lives. Here we’ll discuss some of the typical neuromuscular symptoms a patient with a TBI may experience.
The Three Stages of Recovery
Patients with TBI typically go through three stages of recovery following their accident. The first involves a period of unconsciousness or coma, and can last anywhere from seconds to several weeks or months. Following this there is a second stage of behavioral and memory challenges, such as agitation, disorientation, and amnesia. Lastly, the third stage involves a lengthy period of diverse challenges including behavioral, cognitive, and sensorimotor changes.
Possible Neuromuscular Symptoms
The exact neuromuscular deficit a patient with a TBI will experience depends entirely on the location of the damage within the brain, brainstem, or spinal cord. A patient with diffuse axonal injury affecting many different areas of the brain may have multiple unpredictable motor impairments. On the other hand, a patient with a focal injury involving a specific component of the corticospinal tract may have symptoms that follow an expected pattern depending on exactly which component is damaged. For example, damage to the topmost aspect of the primary motor cortex in the left hemisphere may result in weakness to the right upper limbs (recall what we learned about the motor homonculus!) Overall, long term motor weakness following TBI is relatively rare. However, balance issues are more frequently reported, which can impact patients’ gait and mobility.
| Disorder | Description | Example |
| Dysarthria | Difficulty producing speech due to deficits in the motor system that creates the movements for talking. | Damage to cranial nerve five, the trigeminal nerve, which controls the jaw muscles. |
| Spasticity | Rigidity and increased tone of skeletal muscles | Spasticity may be caused by damage to upper motor neurons in the brain or spinal cord, which causes an imbalance in excitatory and inhibitory signals sent to the lower motor neuron and the muscle. |
| Gait disorders | Abnormalities in limb movements, posture, and/or muscle tone leads causes abnormal walking | Damage to the cerebellum resulting in uncoordinated motor responses can negatively impact gait |
Neuromotor disorders a patient with a TBI may experience.
Ischemic Stroke
Ischemic stroke is large contributor to neuromuscular disability worldwide, and has a profound impact on patients and their families. Ischemic stroke is caused by a blockage in the vasculature within the brain, causing tissue infarction and death. If motor areas of the central nervous system are impacted, there may be permanent disability.
Possible Neuromuscular Symptoms
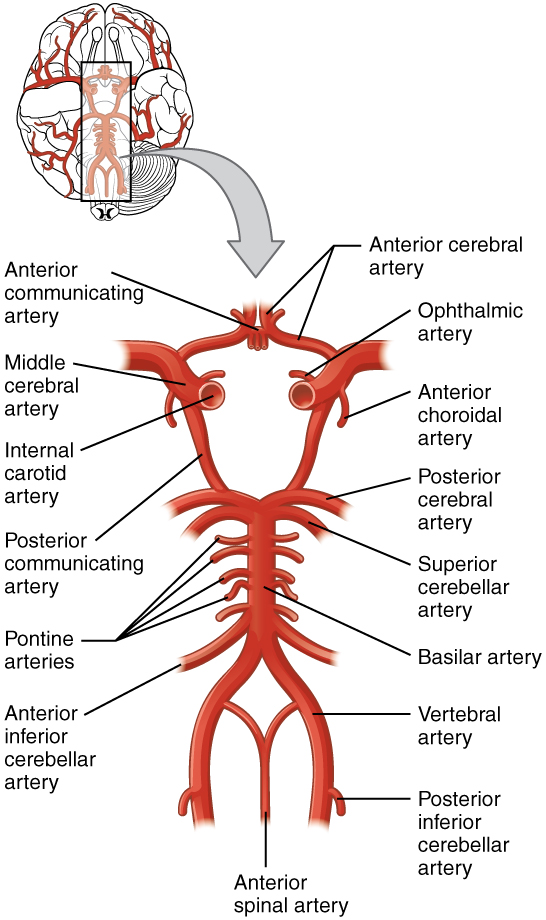
The exact symptoms of a stroke depend on which artery is occluded, causing various “syndromes” with characteristic symptoms. For example, middle cerebral artery syndrome occurs when the middle cerebral artery (MCA) is occluded, and the typical presenting symptoms include hemiplegia and hemianesthesia. Refer back to previous chapters to refresh your knowledge on the vasculature in the central nervous system.
| Clinical manifestation | Description | Location of Occlusion (stroke syndrome) | Anatomical Explanation |
| Aphasia | Disordered speech production and/or comprehension | Left middle cerebral artery occlusion | The middle cerebral artery supplies blood to Broca’s and Wernicke’s areas, which are responsible for speech production and comprehension, respectively. Because the language areas of the brain are located in the dominant hemisphere, aphasia is usually caused by an ischemic event on the left side. |
| Ataxia and gait disorders | Abnormalities in limb movements, posture, and/or muscle tone leads causes abnormal walking | Vertebral-basilar occlusion | Branches of the vertebral arteries supply the cerebellum with blood. When there are occluded, infarction in the cerebellum can alter coordination of movements and alter walking and balance. |
| Left lower extremity paresis | Weakness or paralysis of the left leg | Right anterior cerebral artery occlusion | The anterior cerebral artery supplies blood to the midline portion of the frontal lobe, which includes the motor cortex. Recall the motor homonculus, where the cortical areas that provide function to the upper extremities are in close proximity to the midline. |
Diabetic Peripheral Neuropathy
Diabetic peripheral neuropathy is a complex disease that causes significant neuromuscular disability. Up to 50% of diabetics can expect to develop neuropathy in their lifetime, therefore this condition impacts a large amount of the population.
Distal Symmetrical Polyneuropathy
The most common clinical presentation of diabetic neuropathy is distal symmetrical polyneuropathy. Let’s try to understand this condition by understanding the meaning of each word.
- Distal: away from the center of the body, and is opposite to proximal
- Symmetrical: same on both sides of the body
- Polyneuropathy: damage to many neurons
Therefore, distal symmetrical polyneuropathy begins distally in the feet, involves both sides, and is caused by damage to many peripheral nerves. The condition begins with sensory disturbances in the toes, such as numbness and paresthesia (tingling), which gradually spreads upwards. As the condition progresses, autonomic nerves become involved as well. In severe cases, motor nerves innervating muscles in the most distal part of the lower limbs may be involved, which can lead to muscle weakness and wasting.
Diabetic Foot
Foot complications are common among people with diabetic peripheral neuropathy. Sensory loss in the feet may cause injuries to go unnoticed, which can lead to ulcerations, musculoskeletal (MSK) complications, and, in extreme cases, may require amputation. Foot complications may be prevented by daily foot care and inspections, and by close monitoring by a foot specialist.
References
Baker, J.M. Gait Disorders. (2017) American Journal of Medicine Gait Disorders
Ponsford, J.L. et al. Longitudinal Follow-Up of Patients with Traumatic Brain Injury: Outcome at Two, Five, and Ten Years Post-Injury. Journal of Neurotrauma (2013) Longitudinal Follow up
Katz, J.I. et al. Recovery of Ambulation after Traumatic Brain Injury (2003) Archives of Physical Medicine and Rehabilitation Recovery of Ambulation
Povlishock, J.T., and Katz J. I. Update of neuropathology and neurological recovery after traumatic brain injury. (2005) Journal of Head Trauma Rehabilitation Update of neuropathology
Bradley and Daroff’s Neurology in Clinical Practice (Eighth Edition) Chapters: Ischemic Cerebrovascular Disease and Disorders of Peripheral Nerves
Media Attributions
- corticospinal-tract with exemplars © Rcchang16 adapted by Valerie Swanston & Jennifer Kong is licensed under a CC BY-SA (Attribution ShareAlike) license
- 1314_Circle_of_WillisN © OSCRiceUniversity is licensed under a CC BY (Attribution) license
- Motor_homunculus.svg © Was a bee is licensed under a CC BY-SA (Attribution ShareAlike) license

{kind=link}
{kind=link}