Diabetes Mellitus
Diabetes Mellitus Pharmacology
Diabetes Mellitus Pharmacology
Dylan Mann and Stepheny Zani
Learning Objectives
By the end of this section, you will be able to:
- Classify the major drugs used to manage type 2 diabetes mellitus into groups
- Associate the groups of drugs with their unique mechanisms
Introduction
In general, T2DM pharmacotherapy is aimed at reducing hyperglycemia through increasing tissue sensitivity to insulin, increasing insulin production, or decreasing glucose production and absorption. Additionally, as much as the North American population approaches pre-diabetic levels or has developed T2DM, the management and treatment options continue to grow alongside them. The class of drugs that we will focus in this chapter include GLP-1 receptor agonists, insulin sensitizers, insulin secretagogues, SLGT-2 inhibitors, DPP4 inhibitors, and alpha-glucosidase inhibitors.
GLP-1 Receptor Agonists
The most popular of new T2DM drugs can be grouped as GLP-1 receptor agonists (or GLP-1 analogs). These act by mimicking the effect of the natural hormone GLP-1, and activating GLP-1 receptors. The combined effects of activating GLP-1 receptors exogenously include increased insulin production, decreased glucagon production, slowed gastric emptying, and decreased appetite. All of these effects contribute to stabilizing blood glucose levels in a person with T2DM, and are particularly potent in causing weight loss. However, although touted as miracle drugs by many, there are multiple side effects that persist in the widely available drugs. These include general nausea, stomach pain, and vomiting, primarily due to effects of slowed gastric emptying. Additionally, due to such strong appetite suppression and rapid weight loss, patients often lose significant muscle mass alongside fat loss, especially if insignificant protein and exercise is paired with the medication. It is worth to keep in mind, that GLP-1 receptor agonists are not the first group of drugs prescribed to manage T2DM and that they should be used cautiously and as an add on therapy.

Insulin Sensitizers
Insulin sensitizing drugs have historically been the first class of drugs given to a person with T2DM once diet and exercise are no longer sufficient in managing blood glucose levels. Their main mechanism of action is to reduce the production of new glucose from the liver (reduce gluconeogenesis). Additionally, these drugs cause more glucose transporter proteins such as GLUT4 to embed themselves in the plasma membrane of muscle and adipose tissue, allowing glucose to enter cells at a higher rate. Furthermore, such drugs can decrease glucose absorption in the intestines, resulting in less glucose in the bloodstream. By reducing gluconeogenesis in the liver, increasing insulin sensitivity in the muscle and adipose tissue, and decreasing glucose absorption in the intestines, this class of drugs greatly reduces overall glucose level in the blood. Most common side effects of such drugs include gastrointestinal disturbances such diarrhea, nausea, and abdominal cramps.
Insulin Secretagogues (Sulfonylureas)
Insulin secretagogues or the sulfonylureas class of T2DM drugs act by stimulating the release of insulin from pancreatic beta cells. They work by binding to specific receptors on pancreatic beta cells, and blocking potassium channels. The blocking of potassium channels causes depolarization of the cells, allowing calcium to enter and trigger the release of insulin. The increased release of insulin facilitates the uptake of glucose into tissues and cells, and in turn reduces the amount of glucose in the blood. Because of sulfonylureas direct increase in insulin production, patients must monitor blood glucose levels frequently, and avoid skipping meals to avoid hypoglycemia.
SGLT-2 Inhibitors
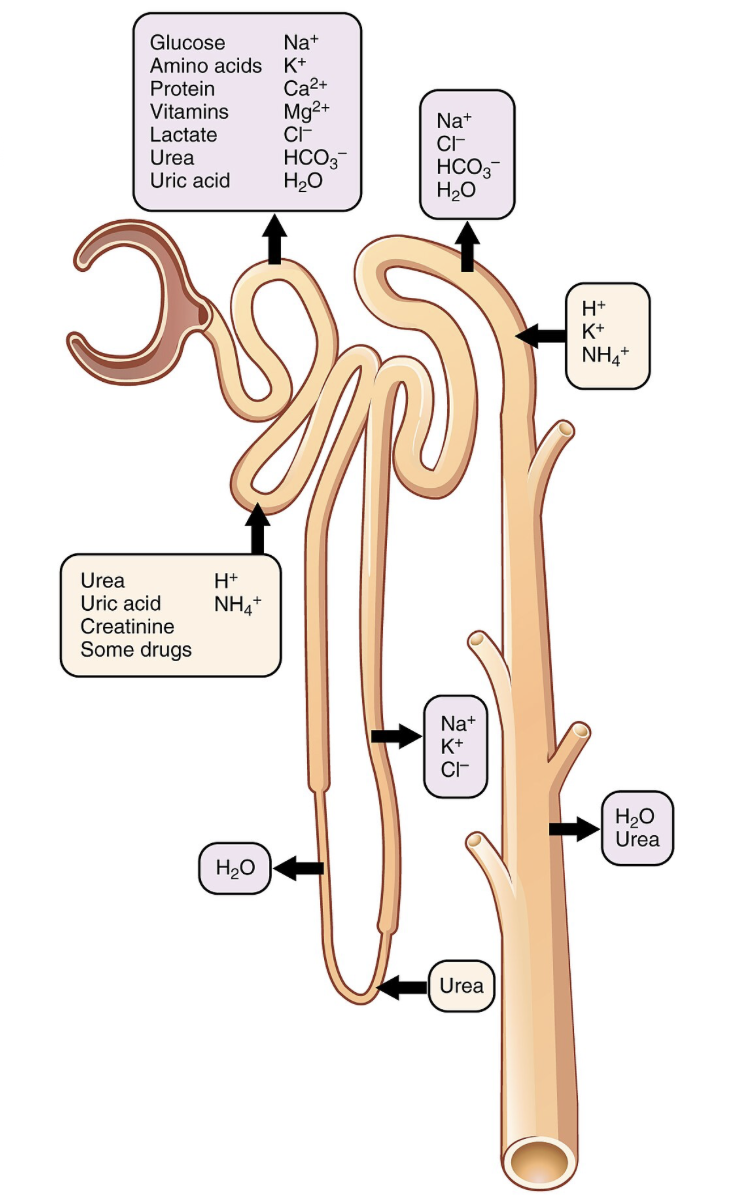
SGLT-2 inhibitors act by inhibiting sodium glucose transport protein 2 (SGLT-2) in the kidneys, which accounts for over 90% of the total renal reabsorption of glucose. When SGLT-2 is inhibited, the kidneys ability to reabsorb glucose back into the blood is greatly limited, and instead glucose is excreted out into the urine. When people with T2DM use SGLT-2 inhibitors, it is hugely important that they consume enough water and nutrients, as common side effects include urinary tract infections, and dehydration. For this class of drugs to work efficiently, renal filtration must be occurring normally, therefore, patients with impaired kidney function might not benefit from this therapy.
DDP-4 Inhibitors
DDP-4 inhibitors are a class of oral T2DM drugs that act by blocking the enzyme dipeptidyl peptidase-4 (DPP-4). Under normal action, DDP-4 breaks down incretin hormones such as GLP-1 and GIP. By inhibiting DDP-4, these hormones are able to circulate the body for extended periods of time. When incretin hormones circulate for longer periods, insulin release is stimulated and glucagon release is reduced for a longer time, both of which contribute to decreasing blood glucose levels.
Alpha-Glucosidase Inhibitors
Alpha-glucosidase inhibitors are a class of T2DM drug that inhibits the enzyme alpha-glucosidase. Under normal conditions, alpha-glucosidase aids in the breakdown of complex carbs into simple carbs such as glucose that the body can easily absorb. If alpha-glucosidase is inhibited, complex carbohydrates are broken down at a slower rate, and glucose absorption is thus slowed down. Overall, alpha-glucosidase slows down digestion, and creates a more gradual onset of glucose after a meal opposed to an otherwise rapid spike.
Section Review
There are many T2DM pharmaceutical therapies, and they all operate under different mechanisms. However, all of such drugs aim to do one thing: reduce blood glucose levels. This may be achieved through multiple mechanisms such as by increasing insulin production, increasing insulin sensitivity, slowing digestion, or inhibiting the breakdown of glucose. With the advancement of knowledge about T2DM and scientific research, more and more options are to become available in the future.
Review Questions
Media Attributions
- Ozempic © Haulin is licensed under a CC BY-SA (Attribution ShareAlike) license
- Metformin is a common insulin sensitizer that is administered orally. Often the class of drug first prescribed to person with T2DM. © Life of a Diabetic is licensed under a CC BY (Attribution) license
- Kidney nephron which which includes the receptor SGLT-2 which accounts for the majority of glucose reabsorption. When inhibited, reabsorption is greatly decreased. © OpenStax College is licensed under a CC BY (Attribution) license

{kind=link}
{kind=link}
{kind=link}