Blood, Anemia, Leukemia, and Blood Tests
Diagnosis of Anemia & Leukemia
Emily Frawley and Jennifer Kong
Learning Objectives
By the end of this section, you will be able to:
- Compare and interpret key hematologic parameters used in diagnosing iron deficiency anemia, including hemoglobin, hematocrit, MCV, MCH, and MCHC.
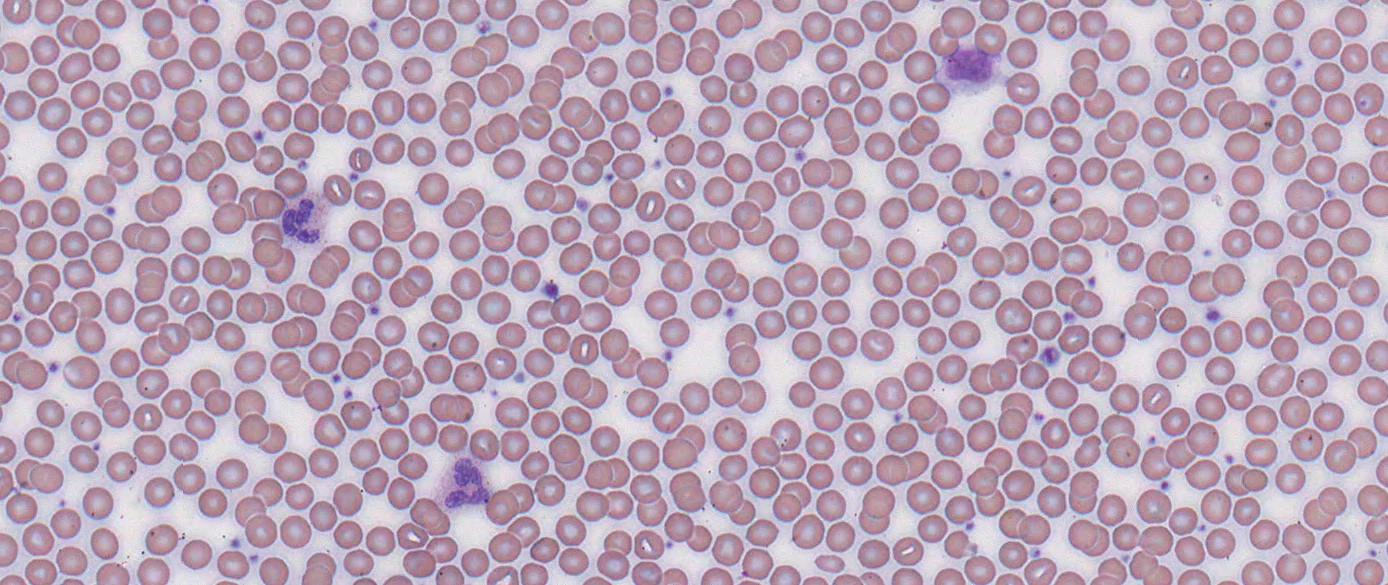
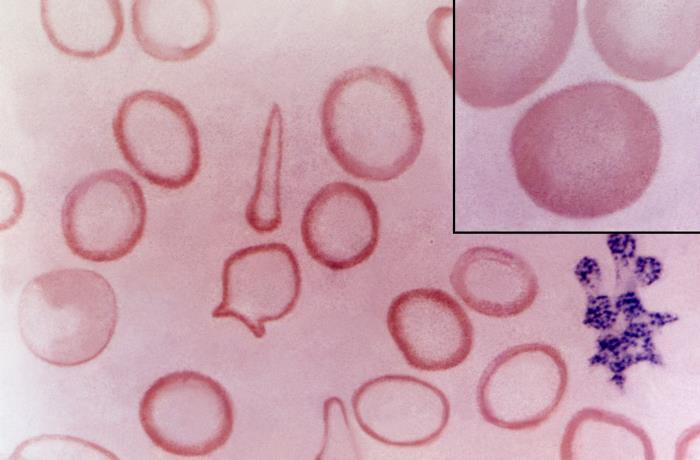
- Identify and interpret typical morphological changes seen in peripheral blood smears in iron deficiency anemia (e.g. microcytosis, hypochromia, presence of pencil cells).
- Describe the role of peripheral blood smear in identifying immature blast cells and distinguishing between different hematopoietic lineages.
- Differentiate between bone marrow aspirate and biopsy, and their respective diagnostic contributions in leukemia.
As mentioned earlier, anemia would have first been detected as part of the hematology test which calculates number and size of RBCs, alongside WBC and platelets. As the health ca
re team explores the cause of the anemia, particularly anemia due to iron deficiency, iron studies will be conducted.
Diagnosis of Iron Deficiency Anemia
Meat in the diet is the primary source of bodily iron (Fe2+ or Fe3+). Hemoglobin and myoglobin are absorbed as heme or inorganic Fe2+ by ferritin and transferrin in the intestinal duodenum. When erythrocytes are destroyed, their iron is recycled in the bone marrow and eventually re-incorporated into forming reticulocytes.
Deficiency disorders arise from two broad categories:
- Increased requirements: infants, children, and pregnant women require more iron in their daily lives
- Increased loss or decreased intake: menstruation in females and bleeding into the GI tract for males can create an iron deficient state, as can nutritional or absorption deficiencies.
Overload disorders are much less common. Hemosiderosis and hemochromatosis are both disorders characterized by increased serum iron, sideroblastic anemia causes iron to accumulate in the mitochondria, and repeated transfusions may cause iron overload.


Two departments in the pathology lab are primarily responsible for assisting in a diagnosis of anemia:
- The Immunochemistry department tests patient serum to directly determine levels of circulating and stored iron present. Serum Iron, Ferritin, and Transferrin are tests commonly used for this purpose.
- Hematology indirectly determines the levels of iron present by evaluating the status of circulating erythrocytes. Hemoglobin levels, Hematocrit, and Red Cell Indices (MCV, MCH, & MCHC) are tests commonly used for this purpose.
Serum iron is found in the ferric (Fe3+) ion form and is bound to transferrin rather than found as free hemoglobin. There is a strong diurnal variation in serum iron so results for this test must be interpreted with caution. Levels are high in the morning, decrease over the course of the afternoon, and are the lowest in the evening. In addition, a patient with iron deficiency may have a normal serum iron and TIBC. (Note: if a sample has marked hemolysis, it must be rejected because a significant free iron is released when a large number of RBCs are damaged. Mild hemolysis has no effect on serum iron testing.)
Ferritin is the major storage form of the ferrous (Fe2+) ion form and is primarily found in hepatocytes and tissue macrophages. It serves as a reserve for the formation of hemoglobin and other proteins. Ferritin levels are a more reliable way of monitoring a patient’s iron status than serum iron as it is not subject to diurnal variation. Ferritin levels will decrease before serum iron levels in iron deficiency scenarios as iron is removed from storage for active use and not replaced.
Transferrin is the transport form of the ferric (Fe3+) ion. It moves iron from it’s storage form of ferritin in hepatocytes and tissue macrophages into the bone marrow where it becomes available for the formation of new erythrocytes. Inflammation or liver damage may cause a reduction in transferrin values.
Transferrin levels may be tested and reported as Total Iron Binding Capacity. TIBC is an indirect measure of how much transferrin is available to carry iron. An increased TIBC indicates more space to take up iron and as such indicates decreased iron levels.
Transferrin saturation is another indirect measure of transferrin and expresses the ratio of serum iron to TIBC. Low saturation indicates decreased iron levels.
Anemia states will be reflected in the size, shape, and color of red cells. A Complete Blood Count will evaluate these indices as a routine and standard part of hematology testing to determine a patient’s Mean Corpuscular Volume (MCV), Mean Corpuscular Hemoglobin (MCH), and Mean Corpuscular Hemoglobin Concentration (MCHC). In addition, a Hematocrit test will evaluate the ratio of plasma volume to red cells.
MCV is an indication of the size of erythrocytes. Microcytes occur when there is not enough iron present in the bone marrow to form full sized erythrocytes. Macrocytes occur due to ineffective erythropoiesis in the bone marrow and are usually due to a deficiency in Vitamin B12, folic acid, and/or folate.
MCH is an indication of how much hemoglobin is contained in the erythrocytes and is expressed in the relative color of the red cell. Hypochromic erythrocytes carry a decreased amount of hemoglobin that can be visualized on the blood smear as a larger than normal center clear area on the red cells. Hyperchromic erythrocytes have a reduced or missing center clear area and are an indication of some form of iron overload.
MCHC is an indication of the concentration of hemoglobin in the erythrocyte relative to its size. It is calculated by dividing the hemoglobin concentration by the hematocrit (MCHC = hgb ÷hct). A decreased MCHC indicates hypochromic erythrocytes are present.
Hematocrit is an indication of the ratio of plasma volume to red cells. A decreased hematocrit indicates a reduction in the number of erythrocytes present in a patient’s blood and is usually due to an anemic state. Note: a relative anemia may occur due to an increase in plasma volume with a normal amount erythrocytes causing a relative decrease in hematocrit.
Diagnosis of Leukemia
As mentioned earlier, the signs and symptoms of leukemia may be manifestations of anemia, leukopenia, and/or thrombocytopenia. Hence the first step in diagnosis is often the patient undergoing a blood test after a visit to their health care provider with complaints of fatigue, pallor, abnormal bleeding or bruising, and/or infection. A blood test would be ordered to examine the mature blood cells in peripheral blood where numbers & types of blood cells are calculated. If these results come back with abnormal values (e.g. abnormally low number of mature RBC, WBC, and/or platelets), a peripheral blood smear will be prepared for examination by a hematopathologist.
Using the peripheral blood smear, the hematopathologist will look at any abnormal cells present that are suggestive of immature, undifferentiated blood cells known as blasts. The hematopathologist will also look for all cell lines to get a sense of which cell lineage is impacted (i.e. myeloid vs lymphoid). At this point, the peripheral blood smear can give results highly suggestive of leukemia but a definite diagnosis can’t be made until cells from the bone marrow can be analyzed.
Bone Marrow Aspirate and Biopsy in Leukemia
The process of bone marrow aspirate vs biopsy is beyond the scope of this text. However, each test gives important information when investigating leukemia. Bone marrow aspiration uses a surgical needle to remove a small amount of fluid and cells from the bone marrow whereas a bone marrow biopsy removes a small piece of bone containing marrow and cells. The advantage of a bone marrow biopsy is that it demonstrates the architecture of bone including marrow cells and possibly infiltration by leukemic cells. Both bone marrow aspirates and biopsy specimens are examined under a microscope.
After examination of the bone marrow, the hematopathologist can give a definitive diagnosis of leukemia and classification. ALL is diagnosed with a bone marrow aspirate of >20% of cells present are lymphoblasts. There will be numerous lymphoblasts with characteristics such as a high Nuclear:Cytoplasm ratio, fine chromatin seen within the nucleus, and numerous vacuolations within the cytoplasm. Ancillary testing, including flow cytometry, and immunohistochemical stains on the biopsy, and cytogenetics/molecular studies may also help with the diagnosis and prognosis.
Upon diagnosis, approximately 90% of children with ALL will be cured with proper treatment[1].
Section Review
To diagnose anemia, a condition of low hemoglobin, iron studies must be undertaken. Iron content in RBCs can be measured either in hematology. The number of red blood cells (hematocrit) and Red Cell Indices (MCV, MCH, & MCHC) are used to determine the amount of iron-containing hemoglobin is present in RBC and how much RBC is present in circulating blood. The amount of iron available – whether as plasma iron, ferritin, or transferrin – is determined using immunochemistry.
To diagnose leukemia, the patients blood sample would have had abnormalities in the hematology tests. When that patient’s sample is identified as such, a blood smear is prepared and human analysis by a medical lab technologist or hematopathologist. If the hematopathologist identifies the presence of numerous blasts in the circulating blood, they will refer the patient to a bone marrow aspirate or biopsy. These tests will analyze the number and type of cells within bone marrow which the presence (or absence) of blasts will help with the diagnosis of leukemia and its classification of lymphoid or myeloid.
Review Questions
Media Attributions
- Empty Blood test vials © kropekk_pl, CC0, via Wikimedia Commons is licensed under a CC0 (Creative Commons Zero) license
- Clinical_Chemistry_Analyzer_,_Клинички_биохемиски_анализатор_3 © Делфина is licensed under a CC BY-SA (Attribution ShareAlike) license
- Peripheral Blood Smear Histology © DHPLC is licensed under a All Rights Reserved license
- iron deficiency anemai © Centre for Disease Control is licensed under a Public Domain license
- https://www150.statcan.gc.ca/n1/pub/82-003-x/2021002/article/00001-eng.htm “Trends in paediatric cancer survival in Canada, 1992 to 2017”by Larry F. Ellison, Lin Xie and Lillian Sung. Statistics Canada ↵

{kind=link}
{kind=link}