Neuromuscular Control of Motion
Pathophysiology of Neuromuscular Control: Muscle Structure and Function (Muscle Strains and Muscular Dystrophy)
Meihua E. Su and Jennifer Kong
Learning Objectives
By the end of this section, you will be able to:
- Describe how muscle fatigue manifests in movement disorders.
- Explain the role of dystrophin and how it relates to muscular dystrophy.
- List some common manifestations of muscular dystrophy.
As already mentioned, movement disorders can occur when there is a dysfunction in nerves, neuromuscular junction, or muscle function. This chapter will focus on muscular disorders that are more benign (e.g. muscle fatigue and strains/sprains) and insidious (e.g. muscular dystrophy).
Muscle Fatigue and Strains
At some point in our active lifestyles, we may have had a muscle problem – whether it be muscle fatigue after a particularly strenuous activity and/or a strain (i.e. tear in the tendon or the muscle itself). In both situations, the anatomy of the muscle itself is normal, but there is an issue with its function. In the case of muscle fatigue, there was a point in time where the muscle did not have sufficient oxygen for efficient aerobic metabolism. As a result, the muscle shifted to anaerobic metabolism which creates lactic acid as a byproduct (assuming oxygen debt was not repaid). As a result, there is physical damage to the muscle tissue from the acidic environment. Similarly, muscle tears also involve physical damage to a localized area. In both situations, the inflammatory response follows, leading to the characteristic features of possible swelling, heat, redness, and pain. While the muscle tissue undergoes inflammation and healing, the function of the muscle is impaired, often manifesting as lack of strength, decreased flexibility, and pain upon use. This would appear as a movement disorder due to the impaired strength and flexibility of the injured muscles. Sometimes, a mobility aid (e.g. crutch) is required to offload weight which lends support to the weaker muscles. However, once the muscle heals, muscular function returns and there is no longer any movement disorder.
Muscular Dystrophy
As mentioned previously, muscle cells have the protein dystrophin to protect myocytes from overstretching and tearing. Dystrophin is a rod-shaped protein that acts like a coil or “shock absorber” at the cellular level. It expands in response to the forces of contraction and stretching to prevent tearing. Muscle strains are the result of physical exertion exceeding the protective capabilities of dystrophin.
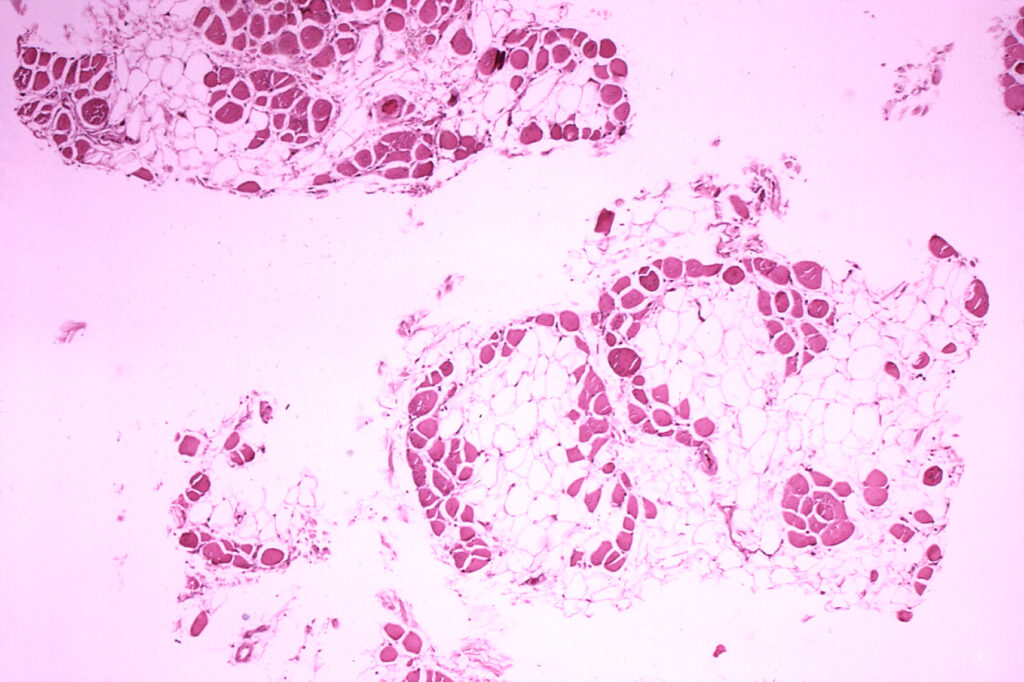
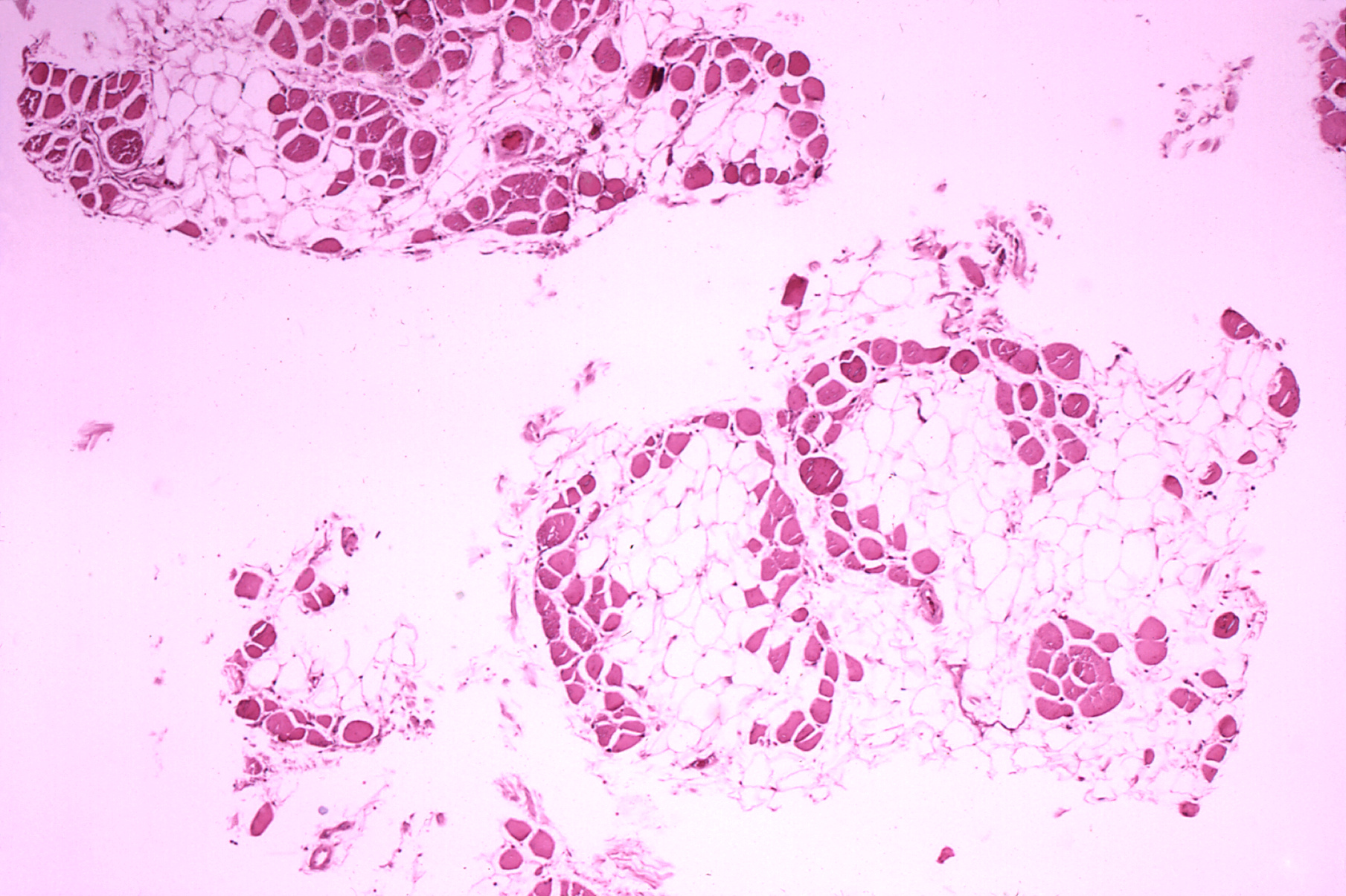
In the genetic condition of muscular dystrophy (MD), the gene for dystrophin contains errors resulting in non-functional dystrophin. Without functional dystrophin, the myocytes lose both their abilities to recoil and to maintain stability and strength during contraction. This results in myocytes being constantly damaged after every use: akin to muscle strains with every use. Inflammation occurs and new myocytes grow to replace the damaged ones. However, the new myocytes also contain dysfunctional dystrophin. Over time, the muscle tissue is replaced with scar tissue and fat due to chronic muscle damage, resulting in loss of muscle strength and function.
There are many kinds of MD, differing in severity, age of presentation, heritability, and affected muscles. However, they share the common feature of defective dystrophin production.
Duchenne and Becker muscular dystrophy (DMD & BMD), are types of “muscular dystrophy,” that leads to a progressive weakening of the skeletal muscles of the upper legs and upper arms due to the lack of dystrophin. In DMD & BMD, muscle contractions cause the cell membrane (sarcolemma) to rupture, causing an uncontrolled influx of ions, especially Ca2+, through the breach. This influx leads to further to cellular damage and a disruption of the environment needed for mitochondrial function and electrical excitability.
DMD/BMD is a sex-linked inherited disorder (abnormal X chromosome) of the dystrophin gene. Because it is X-linked, it presents primarily in males as males rely on that X-chromosome for dystrophin expression. DMD can also manifest in females, but its presentation might take longer to be evident as it is dependent on whether one or both X chromosomes express the defective dystrophin gene. In males, DMD is usually diagnosed in early childhood. For reasons not yet known, BMD presents later in life (adulthood) yet it involves the same gene as DMD. There are many other types of MD which are not sex-linked, meaning that it affects both males and females equally.
MD usually first appears as difficulty with balance and/or motor strength & endurance. If presenting during infancy and childhood, this may manifest in developmental delays in rolling over, sitting up, standing and walking. As muscle tissue is lost, MD presents as easy tiring upon walking, waddling, and wide-based gait (waddling or hip swinging) with arms swings to help maintain balance. MD can progress to an inability to walk if hip and leg muscles are further affected. MD can also affect muscles responsible for breathing, swallowing, and circulation (the heart) which can ultimately cause death due to respiratory failure.
Media Attributions
- Duchenne-muscular-dystrophy © Dr. Edwin P. Ewing is licensed under a Public Domain license

{kind=link}