Atherosclerosis and Angina
Pathophysiology of Atherosclerosis
Tetiana Povshedna
Learning Objectives
By the end of this chapter, you will be able to:
- Identify and explain the main processes that occur during various stages of atherosclerotic plaque development.
- Describe the biological rationale for the most common locations of atherosclerotic plaques.
- Describe common clinical scenarios of atherosclerosis progression.
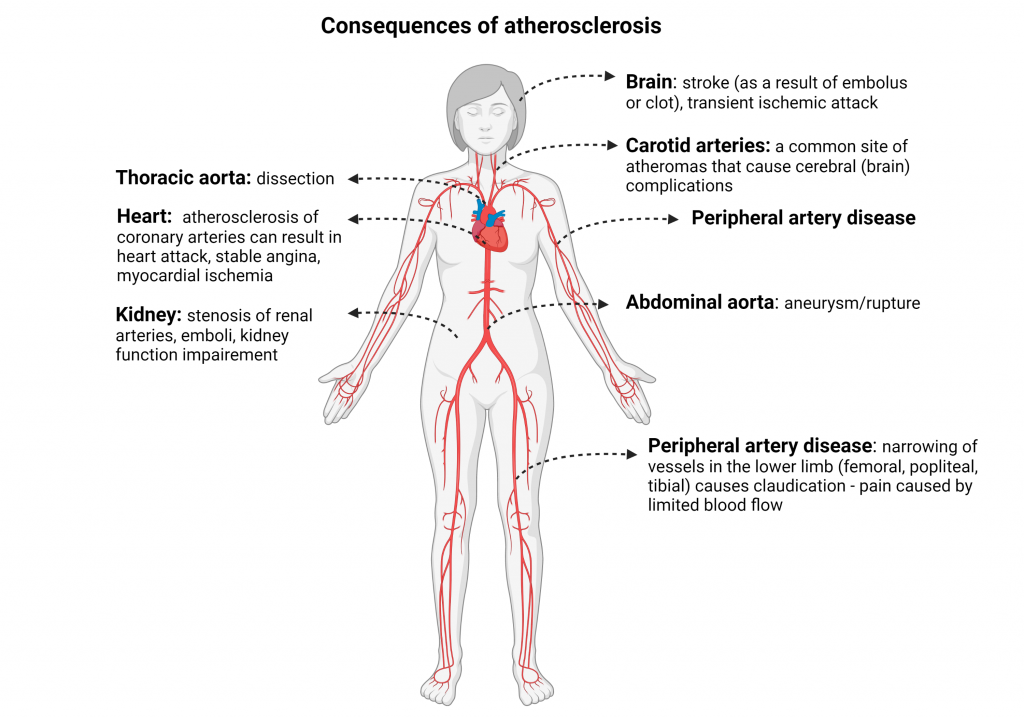
Atherosclerosis develops as a result of a continuous process that involves endothelial activation, lipid accumulation, atheroma plaque formation, vascular remodeling, and ultimate narrowing of the blood vessel lumen. This blood flow restriction due to atherosclerosis can manifest a variety of clinical diagnoses, which are named based on the location of atherosclerotic plaque (heart attack, stroke, and peripheral artery disease )
Atherosclerosis progression is initiated by endothelial activation in response to cardiovascular risk factors, such as hypertension, high blood glucose, smoking, increased cholesterol levels, etc.
Common Locations of Atherosclerotic Plaques
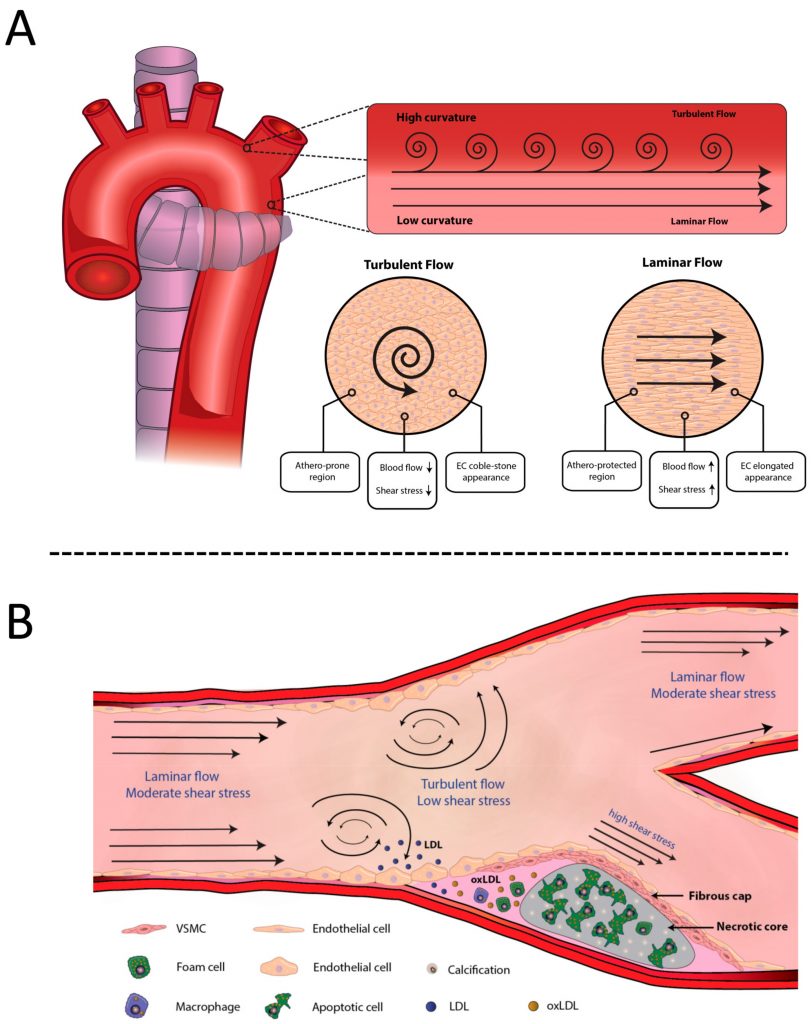
Even though the vascular tree is uniformly exposed to metabolic risk factors, some regions are more likely to form atherosclerotic plaques than others. This phenomenon can be partially explained by mechanical stress (wall shear stress, WSS) and type of blood flow (laminar vs turbulent).
Blood flow disturbance in branching points and bifurcations of the vascular tree results in a specific distribution of atherosclerotic plaques, with the majority of them forming in these common atheroma-prone regions.
This trend highlights the importance of arterial branches and bifurcations in the diagnosis of atherosclerotic lesions.
Some examples of such locations include the bifurcations of:
Stages of Atherosclerotic Plaque Formation
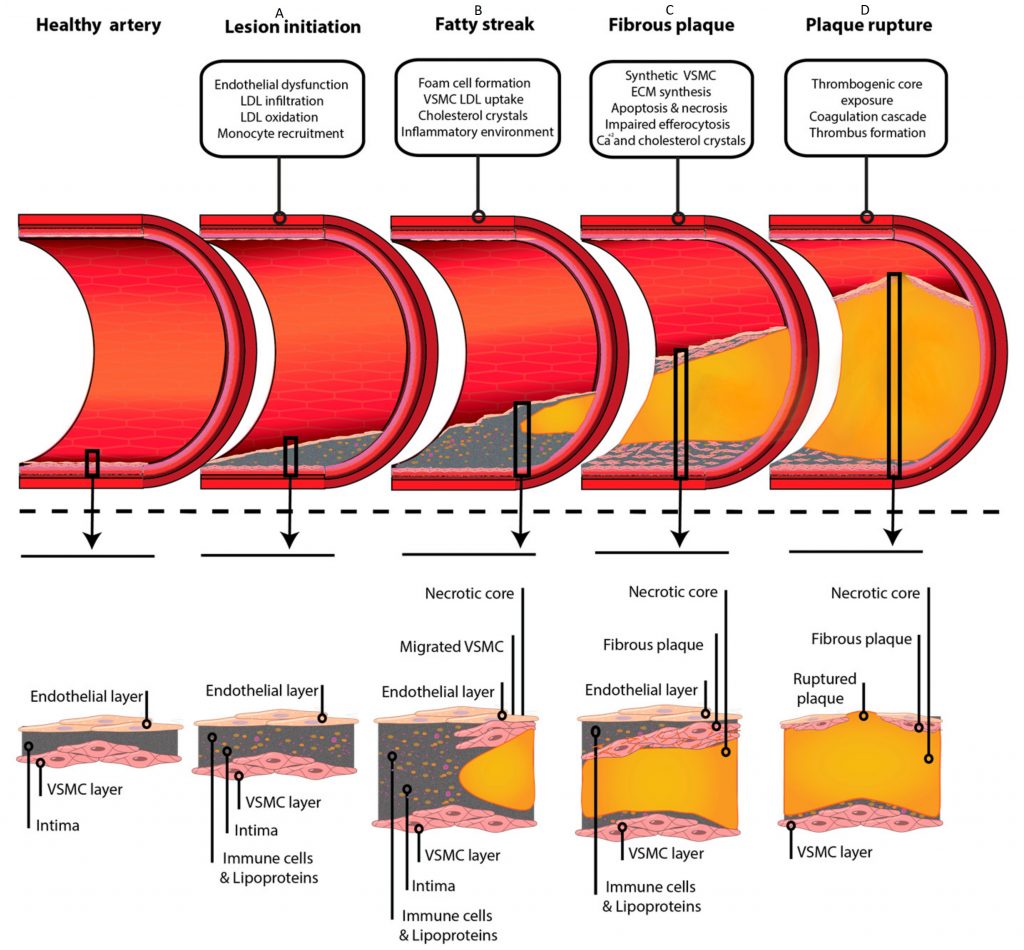
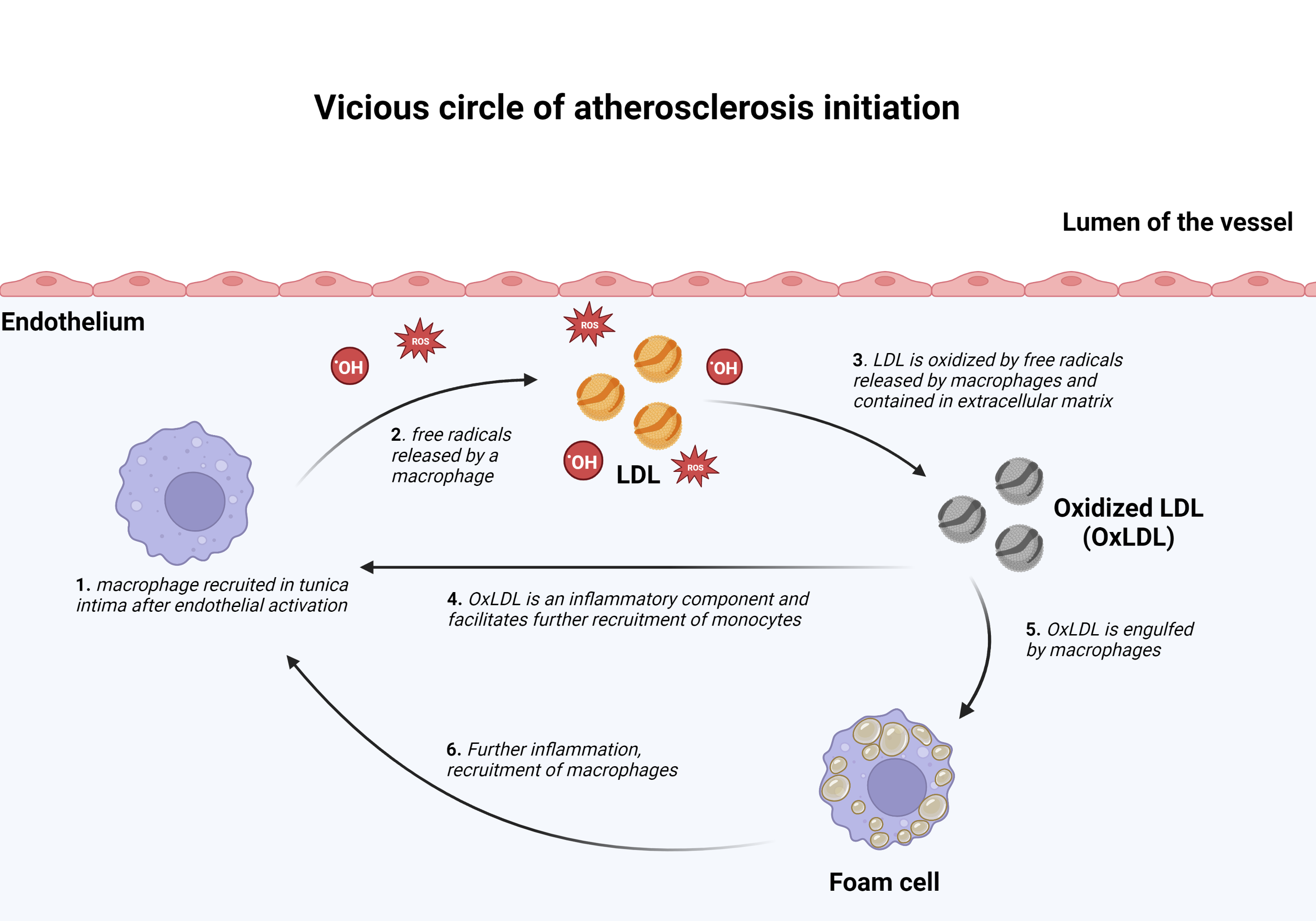
- Lesion Initiation
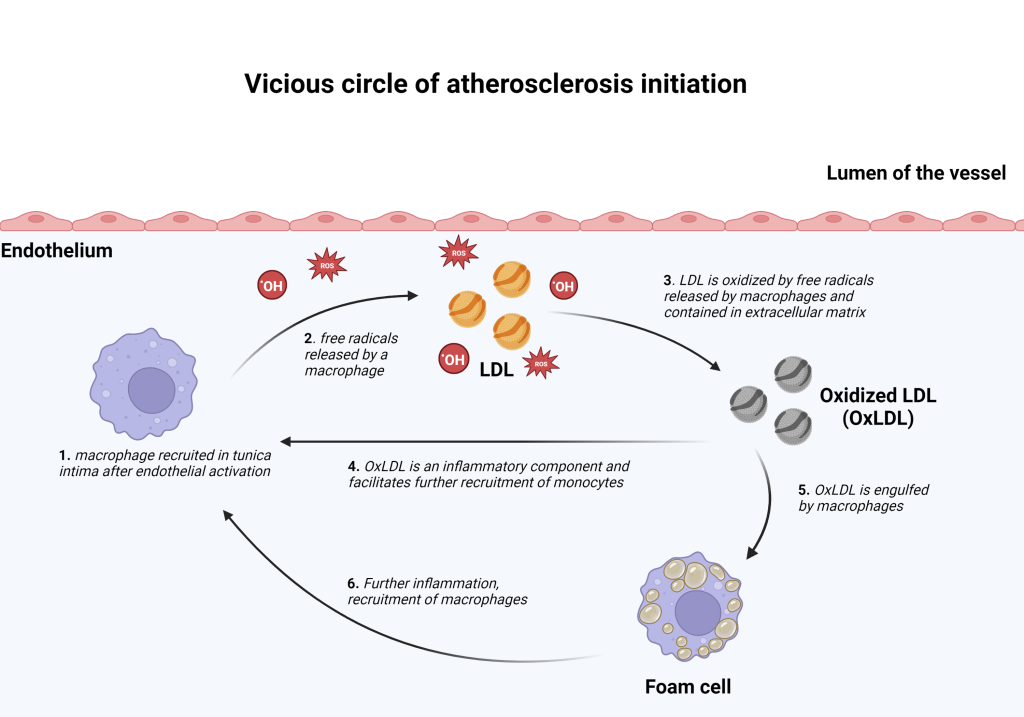
Atherosclerosis plaque formation begins with activation and/or damage to the endothelium, which disrupts the normal process of LDL intake and metabolism. As a result, LDL is modified and accumulated within the tunica intima of a vessel. Endothelial activation/damage affects its permeability, stimulates leukocyte adhesion to its surface, and diapedesis. The leukocytes recruited from the blood into the blood vessel wall are monocytes, that become macrophages once they leave the systemic blood circulation and migrate into tissues.Once within the intimal layer, LDL particles are oxidized by free radicals that are contained in the extracellular matrix and/or produced by recruited monocytes. Oxidized LDL (oxLDL) is a key inflammatory component that facilitates atherosclerosis progression. These initial processes create a “vicious circle” that results in further recruitment of monocytes, LDL retention, and oxLDL accumulation. Recruited monocytes and vascular smooth muscle cells (VSMCs) within the tunica intima engulf oxLDL and become “foam cells” – a name given to these cells because of a foamy appearance of the cytoplasm due to the oxLDL deposition.
2. Fatty Streak
As the “vicious circle” progresses, LDL is deposited both inside cells and in the extracellular matrix, and cholesterol crystals form. The initial lesion increases in size and appears as a visible flat yellow streak on the luminal side of the vessel.
3. Fibrous Plaque
Foam cells (derived from macrophages and VSMCs ) undergo cellular death (apoptosis) and release their contents within the tunica intima. These contents are further engulfed by macrophages in an attempt to “clean” the lesion site. However, an overwhelming amount of oxLDL, dead cells, cholesterol crystals, and extracellular debris form a soft “necrotic” core of growing atherosclerotic plaque. As the lesion progresses, it can accumulate calcium salts and harden over time, impairing the elasticity of blood vessels and their ability to dilate and contract in response to blood pressure fluctuations.
In response to the atherosclerotic lesion progression, more VSMCs are recruited from the tunica media to the intima to form a fibrous cap – a protective layer that covers the necrotic core. Normally, VSMCs facilitate contraction/dilation of blood vessels, but once recruited to tunica intima, they switch towards synthetic activity. VSMCs within the fibrous cap produce a large amount of extracellular matrix (collagen and elastin fibers, proteoglycans) to “cover” the soft necrotic core and stabilize the plaque. The fibrous cap prevents plaque rupture and serves as a barrier between the lumen of the vessel and the necrotic core which, if exposed to the blood flow, can trigger the formation of a blood clot.
4. Outcomes
The thickness of the fibrous cap covering the soft necrotic core of an atherosclerotic lesion, as well as its composition (the amount of collagen/elastin fibers), affect the stability of the plaque and clinical outcomes. As atheroma increases in size, inflammation within the plaque (pro-inflammatory cytokines released by macrophages), as well as inflammatory cytokines in the bloodstream can affect the vulnerability of the plaque.
Atherosclerotic plaques can become more vulnerable if VSMCs within the fibrous cap respond to inflammation by producing enzymes that degrade components of the extracellular matrix, weakening the fibrous cap and making it more susceptible to rupture. A weaker fibrous cap increases the likelihood of the necrotic core getting exposed to the blood flow, which can result in clot formation on top of the plaque.
Key Takeaways
- Circulating monocytes (macrophages once outside of the bloodstream) play an important role in atherosclerosis initiation and progression and undergo morphological changes in the process.
- Inflammation is relevant at all stages of atherosclerosis, from lesion initiation to its rupture.
- Plaque stability determines the likelihood and severity of clinical complications.
Main Scenarios of the Atheroma Progression
- growth of the plaque, progressive obstruction of the blood vessel lumen;
- erosion/rupture of the fibrous cap with subsequent clot formation on its surface;
- plaque/clot disruption and formation of the embolus in the bloodstream;
- increased susceptibility to aneurysm formation ( Similarly to the process within the fibrous cap, extracellular matrix can be degraded within tunica media of the large vessels, weakening the muscular layer and making it more vulnerable to dilatation)
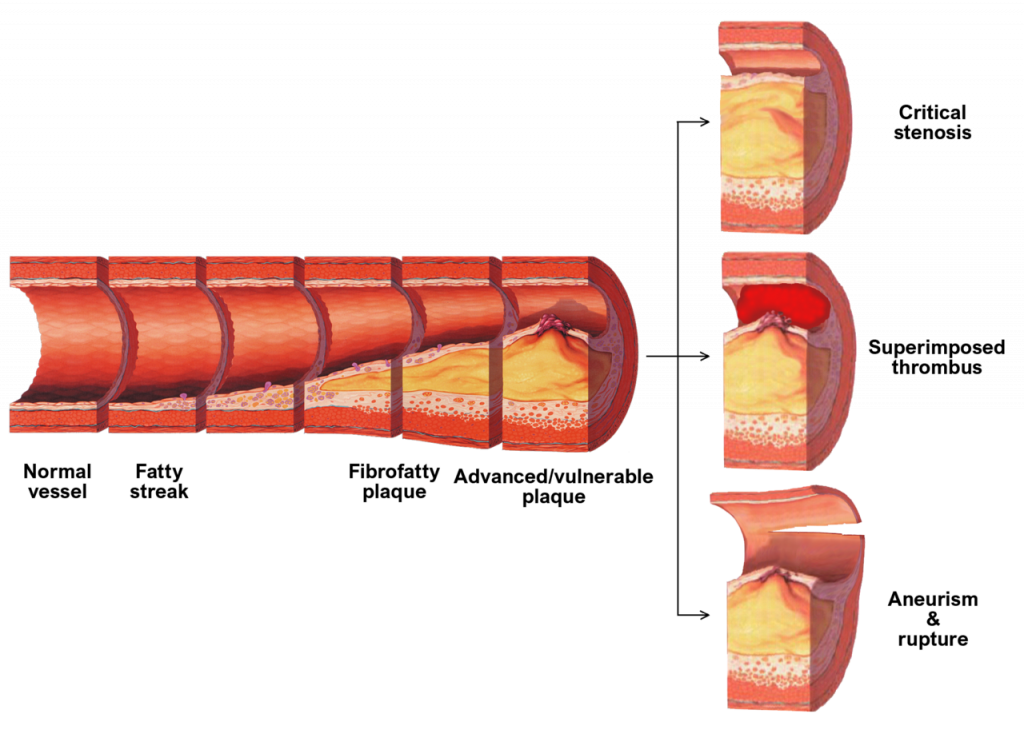
Clinical Scenarios of Atherosclerosis Progression
As mentioned earlier, the distribution of atheromas within the vascular tree is non-random and most commonly occurs at the branching points and bifurcation of large arteries.
As a result, clinical complications of atherosclerosis present as a wide array of symptoms and diagnoses.
Section Review
Microscopic and macroscopic changes that occur during the atherosclerosis progression are summarized below.
Stages of the atherosclerotic plaque formation
Plaque formation stage |
Microscopic changes in the blood vessel wall (histology) |
Outcome |
Macroscopic changes in the blood vessel wall (gross anatomy) |
| 1. Lesion initiation | Endothelial activation in response to risk factors (hypertension, lipid products, cigarette smoke, etc). Recruited monocytes and intimal VSMCs capture oxLDL and become foam cells | Initial LDL oxidation and infiltration within the intimal layer | – |
| 2. Fatty streak | Recruited monocytes and intimal VSMCs become foam cells; cholesterol crystals form within the intima | Intracellular and extracellular LDL deposition | Bright yellow lesions on the luminal surface of the vessel; minimally raised |
| 3. Fibrous plaque | Foam cells, recruited immune cells, and cholesterol crystals form a soft necrotic core. Impaired clearance of apoptotic cells, increased cellular death, and intraplaque hemorrhages facilitate its expansion. VSMCs from media are recruited to the intimal layer, secrete collagen-rich extracellular matrix, and form a protective fibrous cap. |
Formation of the necrotic core and protective fibrous cap; thickness, composition, and collagen content of the fibrous cap determine stability of the plaque | Firm, visible, raised, homogenous, well-marked white areas on the luminal surface of the vessel; sometimes areas of calcification are present |
| 4.1 Plaque rupture/erosion | Erosion (loss of endothelium) or rupture (disturbed fibrous cap) expose the thrombogenic core of the plaque and initiate coagulation | Thrombus formation | Heterogeneous raised lesions associated with surface thrombosis |
| 4.2. Plaque growth | Expansion of the necrotic core increases the size of the plaque | Lumen obstruction | Firm lesions that completely close the blood vessel lumen |
| 4.3. Aneurysm formation and rupture | Weakening of the tunica media might appear as fragmentation in the superficial layers (border between tunica media and tunica intima). Muscular layer of the blood vessel wall can appear condensed, the amount of elastic fibers is decreased | Early stages – ballooning of the vessel wall, later stages – rupture | Rupture of the blood vessel (often fatal) |
References
Jebari-Benslaiman, S., Galicia-García, U., Larrea-Sebal, A., Olaetxea, J. R., Alloza, I., Vandenbroeck, K., Benito-Vicente, A., & Martín, C. (2022). Pathophysiology of Atherosclerosis. International journal of molecular sciences, 23(6), 3346. https://doi.org/10.3390/ijms23063346
https://www.statpearls.com/ArticleLibrary/viewarticle/17943
Review Questions
1. Finish the following sentence. The first step of atherosclerosis lesion initiation is:
- Hypertension
- Lipid deposition within the blood vessel wall
- Endothelial activation/damage
- Clot formation
2. Fill in the blanks with the following words:
deposition, damage, branching points, bifurcations, turbulent, laminar
The most common locations for atherosclerotic plaque formation are _____ and _____ of arteries. This can be related to the type of blood flow as it changes from _____ to _____ , making these regions more prone to epithelial _____ and lipid _____.
3. Fill in the blank.
Macrophages and vascular smooth muscle cells become _____ after engulfing LDL particles.
4. Finish the following sentence. An advanced atherosclerotic plaque consists of:
- Soft necrotic core
- Protective fibrous cap
- A thick layer of smooth muscle
- A dense network of nerve fibers
5. Finish the following sentence. Common outcomes of advanced atherosclerosis DO NOT include:
- Plaque rupture
- Aneurysm
- Clot formation
- Spontaneous lesions reversal
Answer Key
- Endothelial activation/damage
- Branching points/bifurcations, branching points/bifurcations, laminar, turbulent, damage, deposition
- Foam cells
- Soft necrotic core, protective fibrous cap
- Spontaneous lesion reversal
Media Attributions
- atherosclerotic aorta patho © Jebari-Benslaiman, S., Galicia-García, U., Larrea-Sebal, A., Olaetxea, J. R., Alloza, I., Vandenbroeck, K., Benito-Vicente, A., & Martín, C. is licensed under a CC BY (Attribution) license
- Vicious circle © Tetiana Povshedna is licensed under a CC BY (Attribution) license
- atheroma formation © Jebari-Benslaiman, S., Galicia-García, U., Larrea-Sebal, A., Olaetxea, J. R., Alloza, I., Vandenbroeck, K., Benito-Vicente, A., & Martín, C. adapted by Jennifer Kong is licensed under a CC BY (Attribution) license
- Late_complications_of_atherosclerosis © Npatchett is licensed under a CC BY-SA (Attribution ShareAlike) license
- Consequences of atherosclerosis © BioRender adapted by Tetiana Povshedna is licensed under a CC BY-NC (Attribution NonCommercial) license
the narrowing or blockage of arteries that supply upper/lower limbs
elevated blood pressure
type of fluid flow in which fluid travels smoothly
type of fluid flow in which fluid undergoes irregular fluctuations and mixing
part of the blood vessel where it splits in 2 branches
Tissue that lines vessels of the lymphatic and cardiovascular system, made up of a simple squamous epithelium.
low-density lipoprotein, "bad cholesterol" , the form that carries lipids from the liver to various body tissue; increased levels of LDL can accumulate within the blood vessel wall and cause atherosclerosis
(also, tunica interna) innermost lining or tunic of a vessel
cellular component of blood, also known as white blood cells; part of the immune system
movement of blood cells through the blood vessel wall
a type of white blood cell that can further differentiate in macrophages and is involved in adaptive immunity and inflammation
vascular smooth muscle cells
"programmed" cells death that eliminates abnormal cells
middle layer or tunic of a vessel (except capillaries)
small proteins released by cells; allow for communication between the cells involved in the same type of immune response/reaction
unattached mass that travels through the bloodstream and can create blockages, resulting in acute vascular events
abnormal ballooning/ widening of the blood vessel wall cause by it's weakness. Aneurysm rupture is very dangerous and often fatal
widening

{kind=link}
{kind=link}
{kind=link}