Neuromuscular Control of Motion
Pathophysiology of Neuromuscular Control: CNS Issues in the Motor Cortex (Traumatic Brain Injury & Ischemic Stroke)
Valerie Swanston
Learning Objectives
- Describe some of the proposed pathophysiologic changes that contribute to TBI and ischemic stroke.
- Describe the classification of TBI into primary and secondary injury.
- Identify two common etiologies of ischemic stroke.
Exemplar of Damage to Brain (Motor Cortex) or Brain Stem: Traumatic Brain Injury (TBI)
Traumatic brain injury (TBI) is a leading cause of disability and death worldwide, and has a lasting impact on patients and those who care for them. TBIs occur on a spectrum, and their severity can range anywhere from a mild concussion to a severe TBI with lifelong consequences to a person’s function. In Canada, there are approximately 20 000 hospitalizations for TBI every year. TBI commonly arises from motor vehicle accidents, sports, and falls, but can occur anytime there is risk of trauma to the head. Immediate symptoms of a TBI may include nausea, dizziness, memory loss (also called amnesia), and headache. In more severe TBIs, long term symptoms may include altered cognitive and behavioral deficit. Some evidence suggests that severe TBIs may even contribute to the development of neurodegenerative diseases such as Alzheimer’s and Parkinson’s diseases.
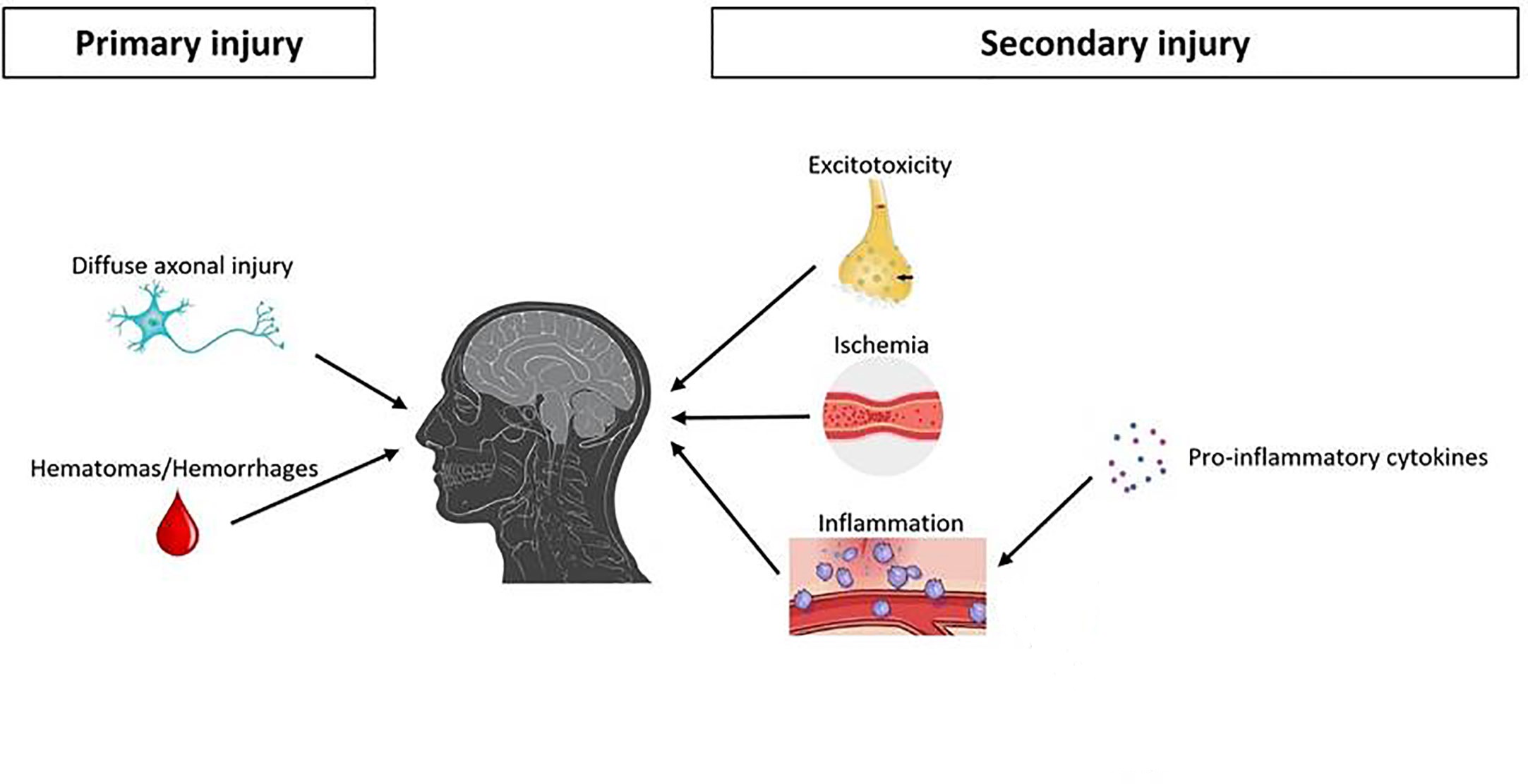
Primary and Secondary Injury in TBI
The progression of a TBI is often divided into two stages: the immediate primary injury and the delayed secondary injury. The primary injury refers to the immediate damage caused to the brain by the traumatic event. In a “closed head” injury, the skull remains intact and injury occurs due to linear or rotational acceleration of the brain colliding with the inner surface of the skull. An example of this would be a head strike from an accident or fall. In a “penetrating” injury an object is embedded into the skull, meninges, or brain tissue. A bullet embedded in the skull as a result of a gunshot wound is an example of a penetrating injury. Damage from a penetrating injury can come as a result of the delicate brain tissue becoming exposed to the external environment.
The secondary injury includes the long-term and slowly progressing changes that occur in the brain as results of the trauma. It is thought that the progression of the secondary injury is the most critical contributing factor to the patient’s recovery.
Pathophysiology of TBI
We certainly don’t know all of the pathophysiologic changes that occur during TBI, and those we have studied are not yet fully understood. The following table outlines some of the possible changes that occur in the brain and it’s surrounding structures, but understand that this list is incomplete and more research is required on this topic.
| Pathophysiological Change | Mechanism |
| Diffuse axonal injury | Direct damage to the neuronal axons within the brain due to destruction of the cytoskeletal network |
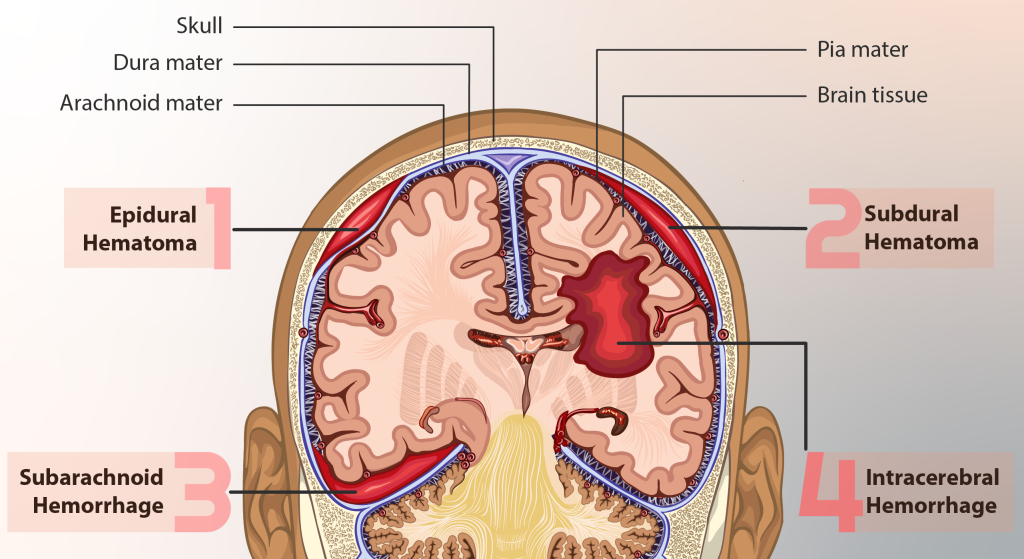
| Hemorrhage | Damage to the blood vessels within the CNS causing bleeding within the brain, which in turn damages tissue and reduces cerebral blood flow to other brain tissue (Figure 12.50) |
| Hematoma | Accumulation of blood in between layers of the meninges causing compression of the underlying brain tissue (Figure 12.50) |
| Brain ischemia | Damage to the vascular endothelial cells in the circulatory system within the CNS results in loss of the brain’s ability to regulate its blood flow. This may cause decreased blood flow to the brain, resulting in a shortage of oxygen in brain tissue, which is clinically called ischemia. |
| Release of excitatory chemical messengers | Damage to the re-uptake transporters for excitatory neurotransmitters such as glutamate causes cellular excitotoxicity, leading to mitochondrial damage and accumulation of damaging reactive oxygen species (ROS) |
| Inflammation | Prolonged release of inflammatory cytokines by the immune system causes disruption to the blood brain barrier, leading to accumulation of excess fluids, which is known as brain edema. If untreated, the excess fluids can cause increased intra-cerebral pressure (ICP), which causes further damage to the brain. |
Pathophysiological mechanisms of brain tissue is injured
Exemplar of Damage to Brain (Motor Cortex) or Brain Stem: Ischemic Stroke
A stroke is a life threatening health emergency that occurs when blood flow to a region of the brain stops, resulting in neuron cell damage and death. Strokes are one of the leading causes of death in Canada; in the year 2019 the incidence of stroke was estimated to be 280 per 100 000 adults aged 20 years and older. There are two broad types of strokes: ischemic stroke and hemorrhagic stroke. Ischemic stroke, which is the focus of this chapter, occurs when a blood vessel within the brain is suddenly blocked, interrupting blood flow. Hemorrhagic stroke, which is comparatively rarer and occurs in approximately 20% of acute strokes, is caused by damage to blood vessels within the brain that leads to significant bleeding into the brain tissue.
Blood Circulation in the CNS
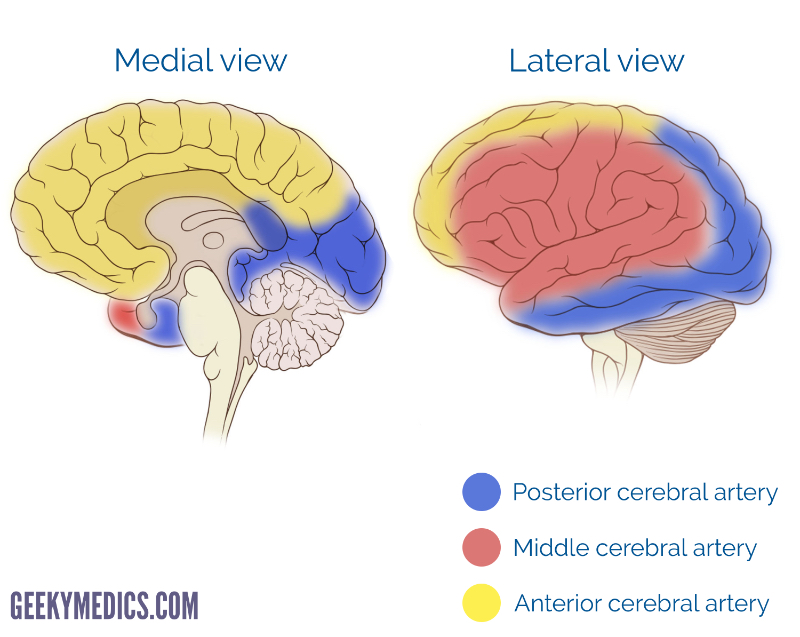
To understand the consequences of a stroke, it’s important to understand the anatomy of the circulatory system within the CNS. Make sure you review the information in Circulation in the CNS. There are three main arteries that supply the cerebral cortex with blood: the anterior, middle, and posterior cerebral arteries. We can use our knowledge of the function of different brain areas in combination with the perfusion area (the area of brain that is supplied with blood) of an artery to work through what the symptoms of an ischemic stroke may be. For example, as the figure below shows, the pre-central gyrus (which contains the motor cortex) is supplied with blood by the anterior and middle cerebral arteries. An ischemic stroke affecting the right middle or anterior cerebral artery will result in motor deficits to the left side of the body (recall what we learned in The Peripheral Nervous System: the motor neurons cross over the innervate muscles on the other side of the body).
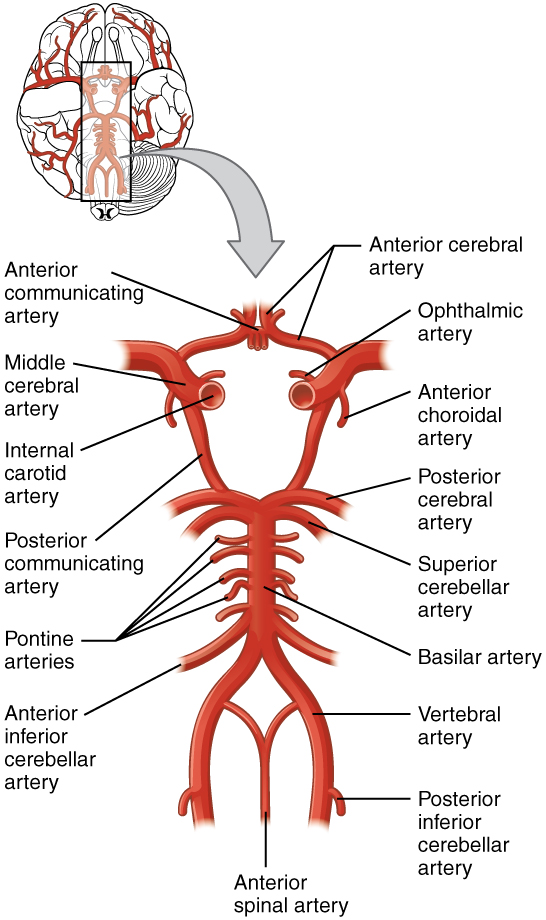
An important anatomical feature of the circulatory system with respect to strokes is a structure called the Circle of Willis. This structure is an anastomosis (connection) of arteries within the CNS that functions to create redundancy within the circulatory system. Essentially, if one artery within the circle becomes blocked, blood flow from other vessels within the circle can accommodate to maintain blood flow and prevent significant ischemia from occurring. This important anatomical feature can prevent significant brain tissue damage in the case of an ischemic stroke.
Causes of Ischemic Stroke
Now that we’ve learned about what an ischemic stroke is, you might be wondering what are the causes of stroke – that is, what actually blocks the blood vessel? We’ll briefly discuss two common mechanisms that can cause an ischemic stroke – cardioembolism and large vessel disease.
Cardioembolism
An embolus is any material that may become lodged and cause a blockage within a blood vessel, called an embolism. Embolisms can be caused by many materials, including fat and air bubbles. When an embolism is caused by a blood clot, is it called a thrombus. In the case of a cardioembolism, the embolus originates in the heart, as suggested by its name. The embolus may travel into the circulation within the CNS, where it can become lodged in a vessel and interrupt blood flow, causing an ischemic stroke. Cardioembolism accounts for approximately 20% of ischemic strokes.
Large Vessel Disease
In large vessel disease, the blockage originates in large vessels such as the internal carotid arteries, aorta, vertebral, or basilar arteries. The most common cause is atherosclerosis, where fatty plaques of cholesterol and other lipids cause narrowing of the vessel. Over time, plaques may rupture and travel to the CNS circulation, causing a stroke. Atherosclerotic plaques are generally caused by diseases of abnormal lipid levels, such as dyslipidemia (high or abnormal levels of blood lipids) or hypercholesterolemia (high blood cholesterol).
Refer to our previous chapter on atherosclerosis to learn about how these fatty plaques originate in the heart, rupture, and then travel to the brain (Atherosclerosis and Angina).
Do you know the signs of a stroke? It could save a life
If you suspect someone is having a stoke, looking for signs with the FAST acronym
- Face: is it drooping
- Arms: can they raise both?
- Speech: is it slurred?
- Time: time to call 9-1-1
References
- Injury in review, 2020 edition: Spotlight on traumatic brain injuries across the life course – Canada.ca
- Richard B. Arbour, Traumatic Brain Injury: Pathophysiology, Monitoring, and Mechanism-Based Care, Critical Care Nursing Clinics of North America, Volume 25, Issue 2, 2013
- Greve, M.W. and Zink, B.J. (2009), Pathophysiology of traumatic brain injury. Mt Sinai J Med, 76: 97-104. https://doi.org/10.1002/msj.20104
- Sulhan, S., Lyon, K.A., Shapiro, L.A., Huang, J.H. Neuroinflammation and blood–brain barrier disruption following traumatic brain injury: Pathophysiology and potential therapeutic targets. J Neuro Res. 2020; 98: 19– 28. https://doi.org/10.1002/jnr.24331
- Akhaddar, A. (2021). Review of Craniospinal Acute, Subacute, and Chronic Subdural Hematomas. In: Turgut, M., Akhaddar, A., Hall, W.A., Turgut, A.T. (eds) Subdural Hematoma. Springer, Cham. https://doi.org/10.1007/978-3-030-79371-5_1
- Thapa, K., Khan, H., Singh, T.G. et al. Traumatic Brain Injury: Mechanistic Insight on Pathophysiology and Potential Therapeutic Targets. J Mol Neurosci 71, 1725–1742 (2021). https://doi.org/10.1007/s12031-021-01841-7
- Canadian Chronic Disease Surveillance System (CCDSS) (canada.ca)
- Bradley and Daroff’s clinical neurology in practice, Ischemic cerebrovascular disease chapter (Ischemic Cerebrovascular Disease – ClinicalKey)
- Ischemic Stroke – ScienceDirect
- Hemorrhagic stroke – ScienceDirect
- 64-03-22-3069-Stroke in Canada Infographic-EN-FINAL (fast acronym)
- Stroke – Canada.ca
Media Attributions
- brain hemorrhage © MyUpchar adapted by Valerie Swansto is licensed under a CC BY-SA (Attribution ShareAlike) license
- TBI is licensed under a CC BY (Attribution) license
- cerebral-vascular-territories © Frank Gaillard. Patrick J. Lynch is licensed under a CC BY (Attribution) license
- 1314_Circle_of_WillisN © OSCRiceUniversity is licensed under a CC BY (Attribution) license

{kind=link}