Autoimmunity
Vitiligo
Vitiligo
Dylan Mann and Morgan Alford
Learning Objectives
By the end of this section, you will be able to:
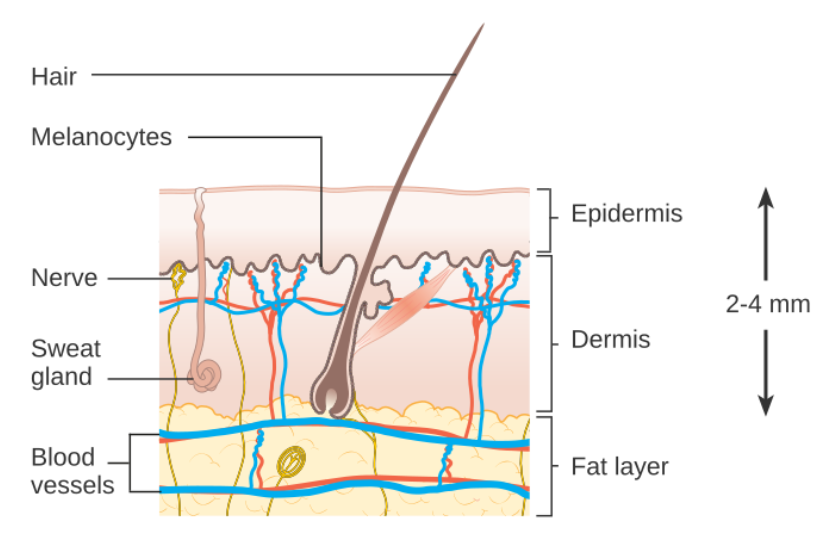
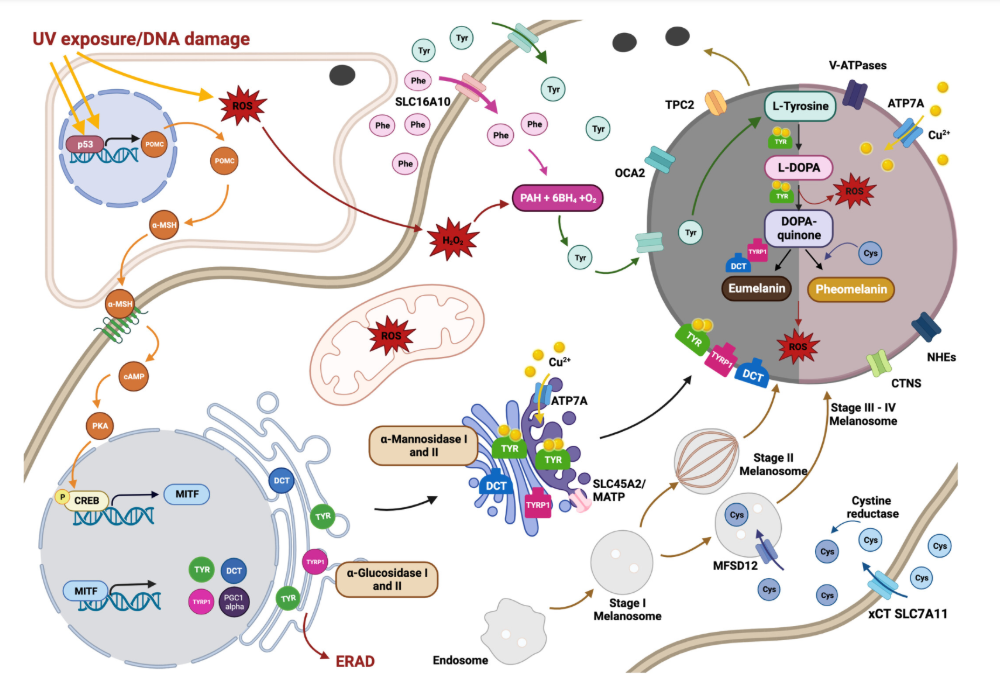
- Describe the basics of skin anatomy and the key players in the melanin production pathway.
- Distinguish between segmental and non-segmental vitiligo based on mechanism and incidence rate.
- Describe the autoimmune aspect of vitiligo development and action.
- Explain vitiligo diagnoses, treatment options and their mechanisms of action.
Introduction and Classification

Skin Anatomy
Melanin Production and Metabolism
Vitiligo Pathogenesis
Diagnosis and Treatment
Vitiligo diagnosis is primarily made by visual inspection of the skin. Observations of localized hypopigmented skin patches can often be made by the naked eye, although tools such as a Woods lamp can be useful for further inspection. A Woods lamp shines long wave ultraviolet light, and in the absence of other light, it makes patches and boarders of vitiligo lesions exceptionally clear. Blood tests are also a useful tool in vitiligo diagnosis, particularly in ruling out the possibility of other skin conditions causing depigmentation. Blood examination would test for the presence of antibodies and vitamin deficiencies which could cause skin abnormalities not associated with vitiligo diagnosis. It is worth noting that vitiligo is often underdiagnosed or misdiagnosed depending on people’s ethnicity or skin tone. People with darker skin may be hastily diagnosed with vitiligo despite the possibility of other skin depigmentation mechanisms. In contrast, people with lighter skin are often undiagnosed or do not seek medical attention when patches are found.
Vitiligo treatment has historically depended on the size of hypopigmented areas. If the areas are small, cosmetic coverup or topical immune suppressants may be applied. Topical immunosuppressants, such as the promising new drug Opzerula, act by altering the immune system in the skin only, opposed to the entire immune system. Such drugs can reduce or prevent the activity of T cells or cytokines, resulting in a reduction of inflammation and risk of melanocyte breakdown.
If the areas are large, systemic immune suppression, skin bleaching, or skin grafts may be used. Systemic immune suppressant drugs include corticosteroids such as Prednisone, Betamethasone, and Dexamethasone. Such drugs can reduce the activity of the entire immune system, resulting in the slowing or complete prevention of melanocyte destruction. However, if such drugs are used, close monitoring from a medical professional is necessary, as increased risk of dangerous infection and other complications become prevalent.
In all cases of vitiligo, it is crucial for patients to wear sunscreen, as depigmented skin lacking melanin is especially vulnerable to burns and UV radiation, which may result in skin cancer (Melanoma). Today, there is an increasing movement towards embracing the cosmetic effects of vitiligo and redefining conventional beauty standards. Because vitiligo does not inherently impose health risks, other than increased risk of UV damage, many individuals have opted out of therapeutic regimes.

Review Questions
Media Attributions
- Example non-segmental vitiligo in a patient hands © Tor Langeland is licensed under a CC BY-NC (Attribution NonCommercial) license
- Diagram of the skin and its layers. © Cancer Research UK is licensed under a CC BY-SA (Attribution ShareAlike) license
- In depth view of melanin production pathway. © Synman et al. is licensed under a CC BY-NC-ND (Attribution NonCommercial NoDerivatives) license
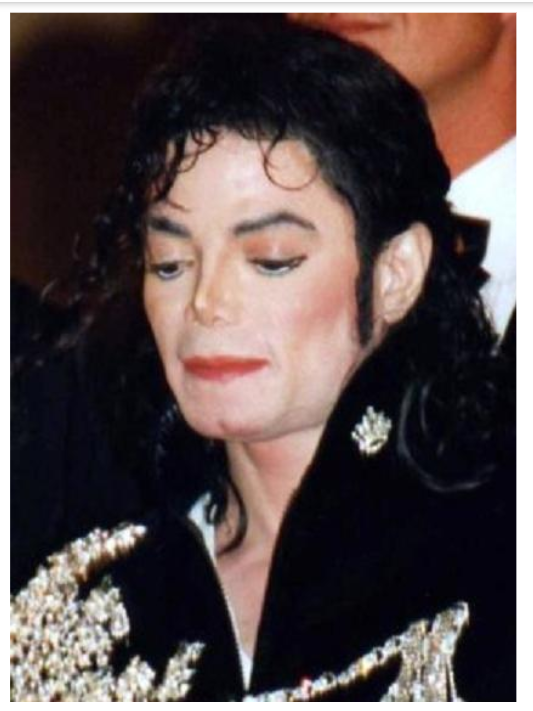
- Michael Jackson, undoubtably the most famous person with vitiligo. Jackson used both skin grafts and cosmetic makeup to aid his condition. © Georges Biard is licensed under a CC BY-SA (Attribution ShareAlike) license
- Winnie Harlow is a world famous fashion model with vitiligo. She is a spokesperson in the ongoing movement of vitiligo representation and awareness. © Georges Biard is licensed under a CC BY-SA (Attribution ShareAlike) license
genes part of the major histocompatibility complex
normal components of an individual's own body that are mistakenly targeted by the immune system
cell of the adaptive immune system that binds APCs via MHC II molecules and stimulates B cells or secretes cytokines to initiate the immune response
adaptive immune cell that directly kills infected cells via perforin and granzymes, and releases cytokines to enhance the immune response
specialized lymphocyte that suppresses local inflammation and inhibits the secretion of cytokines, antibodies, and other stimulatory immune factors; involved in immune tolerance
multiprotein complexes that activate inflammatory responses
small proteins released by cells; allow for communication between the cells involved in the same type of immune response/reaction

{kind=link}
{kind=link}
{kind=link}