Chapter 10. Tubes and Devices
10.3 Nasogastric Tubes
Using a Nasogastric Tube
A nasogastric (NG) tube is a hollow flexible plastic or silicone tube inserted through a nare, past the nasopharynx, oropharynx and into the stomach or the upper portion of the small intestine (the later referred to as naso-jejunum). NG tubes are used for feeding, gastric decompression, or gastric lavage.
An NG tube used for feeding is usually softer and has a smaller lumen than tubes used for gastric suctioning / decompression. NG feeding tubes are used for patients who may have swallowing difficulties or require additional nutritional supplements. Placement of blindly inserted enteral tubes must be verified by x-ray before initial use for feedings or medication administration (Bourgault et al., 2014). Blindly inserted means there has not been direct visualization that the tube in the correct position.
Sometimes normal peristalsis is interrupted (i.e., post op, in association with certain conditions). In these situations a naso gastric tube is used for gastric decompression. Removal of gastric contents can be done either by gravity or by being connected to a suction pump. In these situations, the NG tube is used to relieve gastric distention and in doing so prevent nausea and vomiting. In the event a patient swallows toxic substances, a nasogastric tube can be inserted and used to lavage or wash the stomach of its contents. NG tubes for these purposes generally have a larger lumen than tubes used for feeding purposes (Perry et al., 2018). Sometimes referred to as a Salem Sump or Levin, these tubes are double lumen. The main lumen is attached to suction, the second lumen acts as an air vent which prevents suctioning of gastric mucosa when the stomach is empty.
When working with people who have nasogastric tubes, remember the following care measures:
- There is potential for pressure injury at the nares and in the mucosa. The tube constantly irritates the nasal mucosa. Ensure that the tube is securely anchored to the patient’s nose to prevent excess tube movement, and is secured to the gown to avoid excessive pulling or dragging.
- There is potential for nasal and mouth dryness and discomfort. Because one nostril is blocked, patients tend to mouth breathe. This can cause drying of the nasal and oral mucosa, and patients will complain of thirst, but they are usually NPO (nil per os, or nothing by mouth). Provide mouth care frequently. This can include rinsing the mouth with cold water or mouthwash as long as the patient does not swallow. Silicone based mouth care products are helpful for some. Some patients may be allowed to suck on ice chips.
- Potential for tube obstruction resulting in abdominal pain, discomfort, nausea, or vomiting. In such cases the nurse must investigate complaints of these things immediately, ensuring the drainage flow is not obstructed and to determine if the tube needs to be irrigated.
- Risk of aspiration. Persons with these tubes should never be allowed to lie completely flat. Lying flat increases the patient’s risk of aspirating stomach contents. The head of bed should always be raised 30 degrees or higher (consult agency policy).
- Potential for tube migration. Ensure tape is secure on the tube and nose or face. Measure and record the external length and compare to previous measurements.
- If used for decompression, assess GI function including secretion volume, character, and pH (Perry et al., 2018).
- NG tubes used for decompression: Set suction as ordered or low if not specifically ordered
- Tubes that appear plugged from medications or tube feed may require declogging (consult agency guidelines).
- Check agency policy for checking tube placement, which may include:
-
- X-ray. This is the gold standard for NG tube verification (Stewart, 2014).
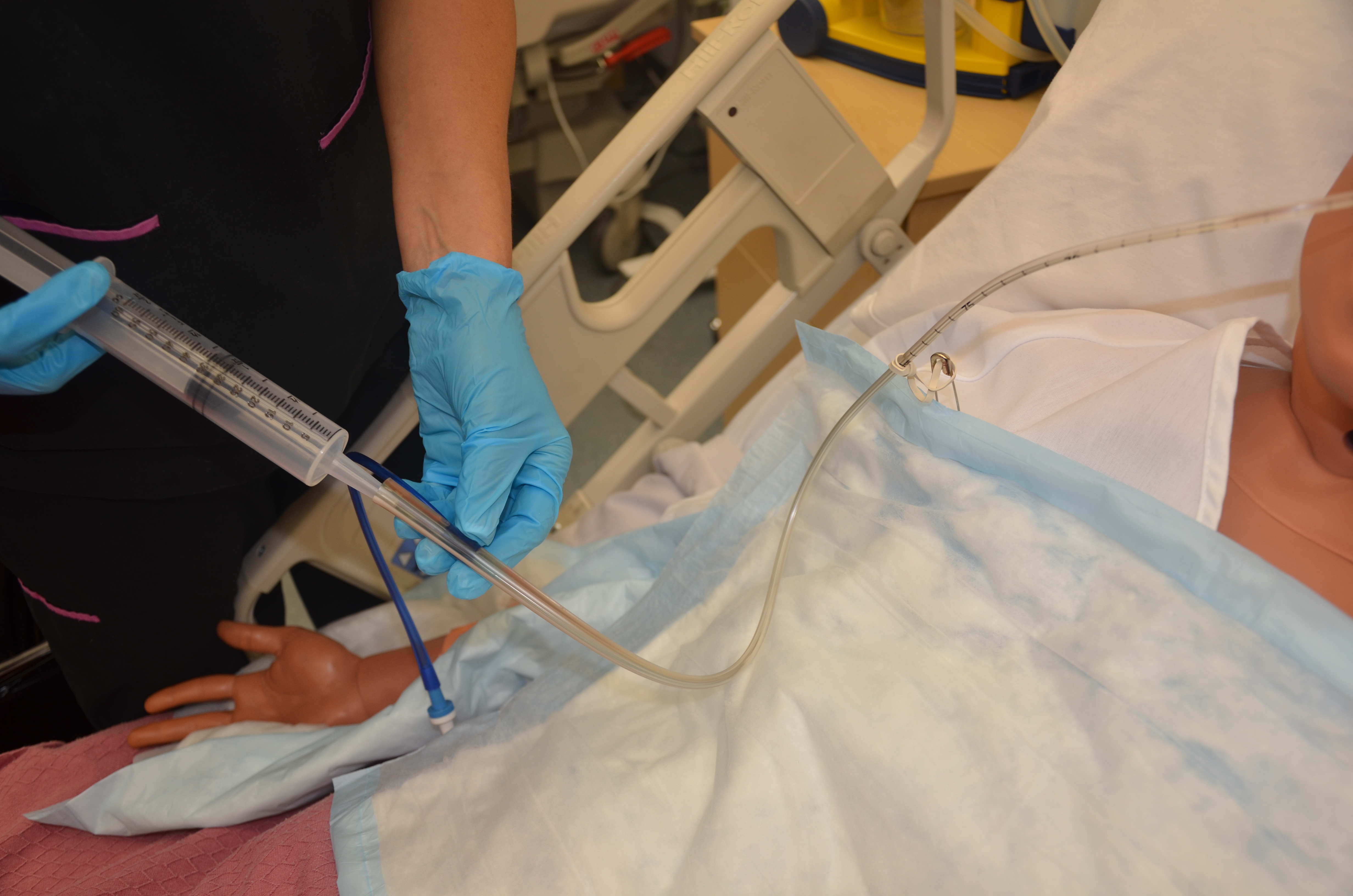
- Gentle aspiration with a syringe to observe gastric contents for amount, colour, and quality. Gastric contents can be green, off white, tan, bloody, brown, or yellow.
- Use pH paper to measure pH of aspirate. Keep in mind that certain medications can alter gastric pH making this part of the assessment unreliable for some patients (Lilley et al., 2016). pH alone cannot accurately distinguish between gastric and respiratory placement. Radiographic confirmation may still be necessary (Perry et al., 2018).
- External length when recorded, assessed frequently and compared with current readings helps to establish tube migration.
- Know the patient’s history: Persons with recent gastric surgery cannot have NG tubes inserted or reinserted blindly.
Checklist 80 outlines the steps for inserting a nasogastric tube.
Checklist 80: Inserting a Nasogastric Tube—AdultDisclaimer: Always review and follow your agency policy regarding this specific skill. |
|||
Safety considerations:
|
|||
Steps |
Additional Information |
||
| 1. Perform hand hygiene. Check prescriber’s orders for type of NG tube to be placed and reason for placement. Gather supplies. | This prevents the transmission of microorganisms. Check appropriate orders relevant to patient safety.
Supplies include NG tube, lubricant, towel, tape securement device, catheter tip syringe, cup of water with straw. If no specific order for NG tube size, use your nursing judgment: large lumens→decompression; small lumens→feeding. 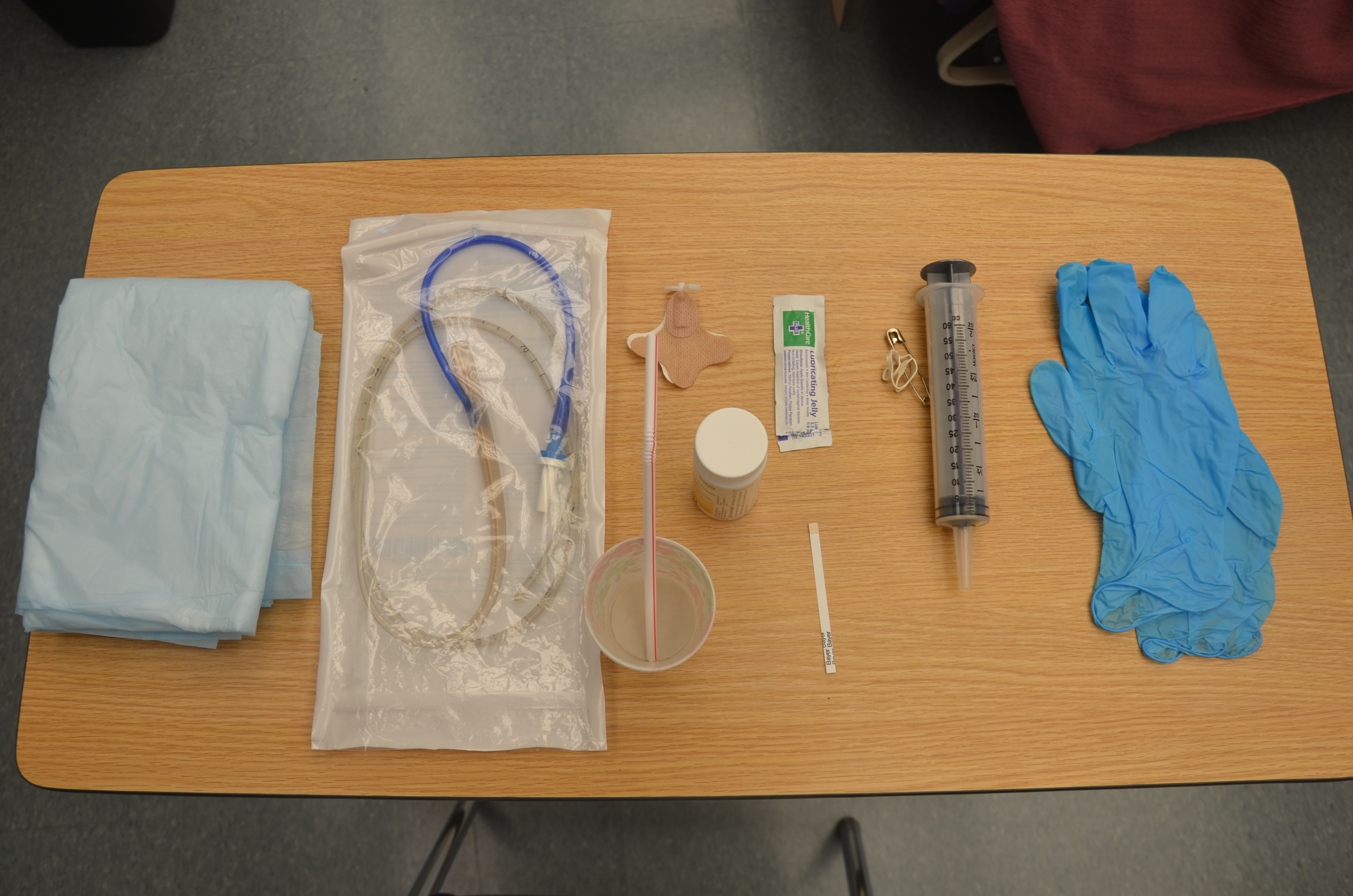 |
||
| 2. Assess patient’s level of consciousness and understanding of procedure. | Patient must be able to follow instructions related to NG insertion to allow for passage of tube through nasal and gastrointestinal tracts. | ||
| 3. Visually inspect condition of patient’s nasal and oral cavities. | Check for signs of infection or skin breakdown. If the patient is at risk for intracranial passage of the tube (i.e., basilar skull fracture) avoid the nasal route. Consult prescriber for alternate route. | ||
| 4. Palpate patient’s abdomen for distension, pain, and/or rigidity. Auscultate for bowel sounds. | Document assessment findings and determine appropriateness of NG tube insertion related to reason for insertion and patient’s physical assessment. | ||
| 5. Apply clean gloves. Assess for the best nostril before you begin. Do this by occluding one side and asking the patient to sniff. Ask the patient about previous injuries or history of a deviated septum. | If either nostril is equally suitable, select the nostril closest to the suction.
 |
||
| 6. Position patient sitting up at 45 to 90 degrees (unless contraindicated by the patient’s condition), with a pillow under the head and shoulders. | This position allows the NG tube to pass more easily through the nasopharynx and into the stomach. | ||
| 7. Raise bed to a comfortable working height. | This helps prevent biomechanical injury to the healthcare provider. | ||
| 8. Explain the procedure to the patient. Agree on a signal the patient can use if they wish you to pause during the procedure. | This procedure can be anxiety-provoking and uncomfortable for many patients. Providing a means for the patient to communicate discomfort and a desire to pause during the procedure helps alleviate anxiety. | ||
| 9. Place a towel on the patient’s chest and provide facial tissues and an emesis basin. | Nasal and oral secretions may be evident during the procedure. | ||
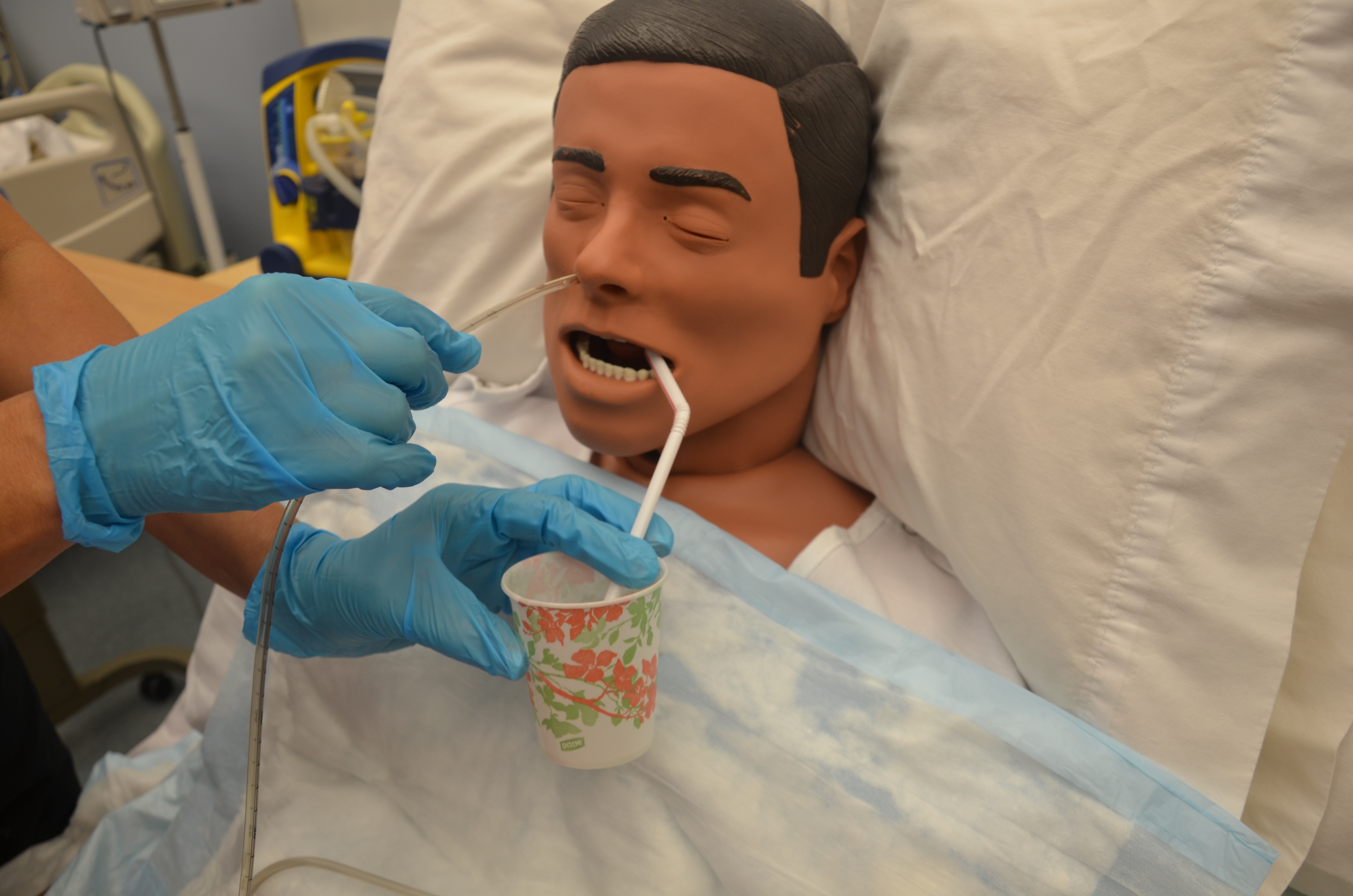
| 10. Provide patient with drinking water and a straw if the patient is not fluid restricted and can hold the cup. | Sipping water through a straw helps to initiate the swallowing reflex and facilitate passing of NG tube. | ||
| 11. Stand on patient’s right side if you are right-handed and the left side if you are left-handed. | You will use your dominant hand to insert the tube. | ||
12. Measure distance of the tube from:
and then mark the tube at this point. Note: Add 20 to 30 cm for an NJ tube.
|
This determines the appropriate length of NG tube to be inserted.
  |
||
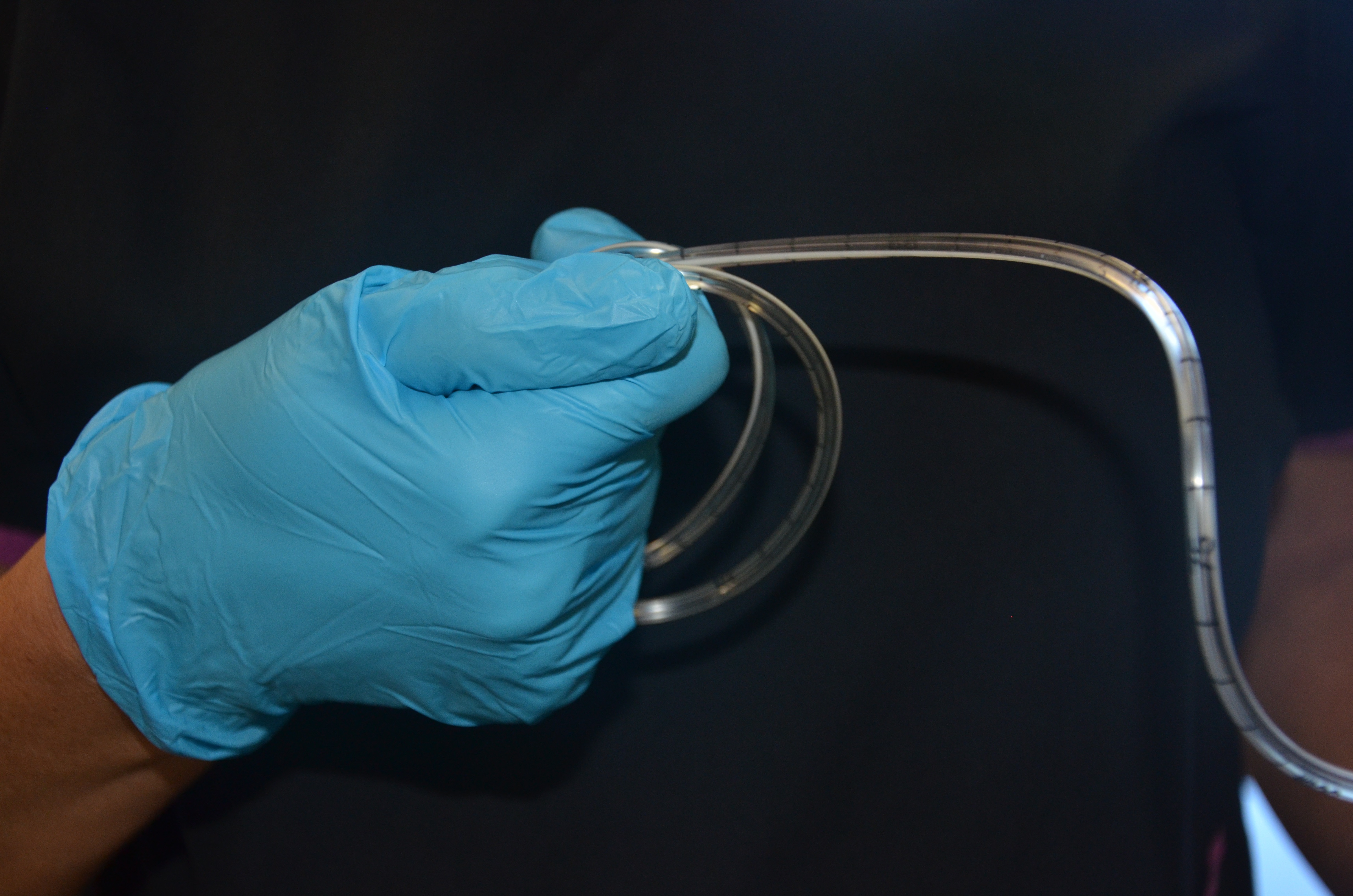
| 13. Curve 10 to 15 cm of the end of the NG tube around your gloved finger, and then release it. | Curling the NG tube around your finger helps it conform to the normal curve of the nasopharynx.
|
||
| 14. Lubricate NG tube tip according to your agency policy (often approx 10 cm).
If inserting a weighted feeding tube with a stylet or guidewire, follow manufacturer’s instructions for lubrication (often involves injecting water into in) Prepare securement device. |
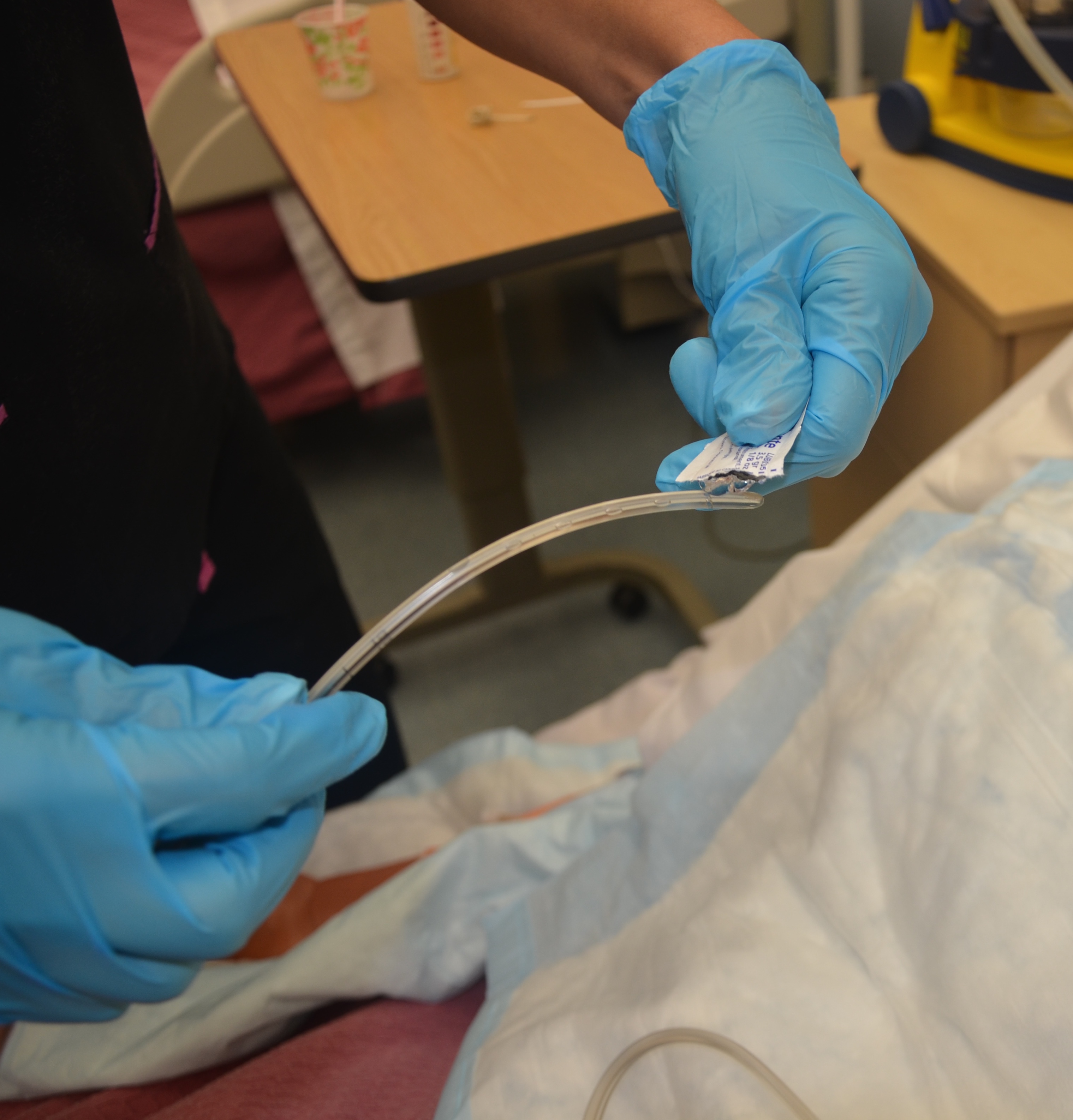 Never use non-water-soluble lubricant (e.g., Vaseline), as it will not dissolve and may cause respiratory complications if it enters the lungs. Agency policy might restrict who can insert a weighted feeding tube. |
||
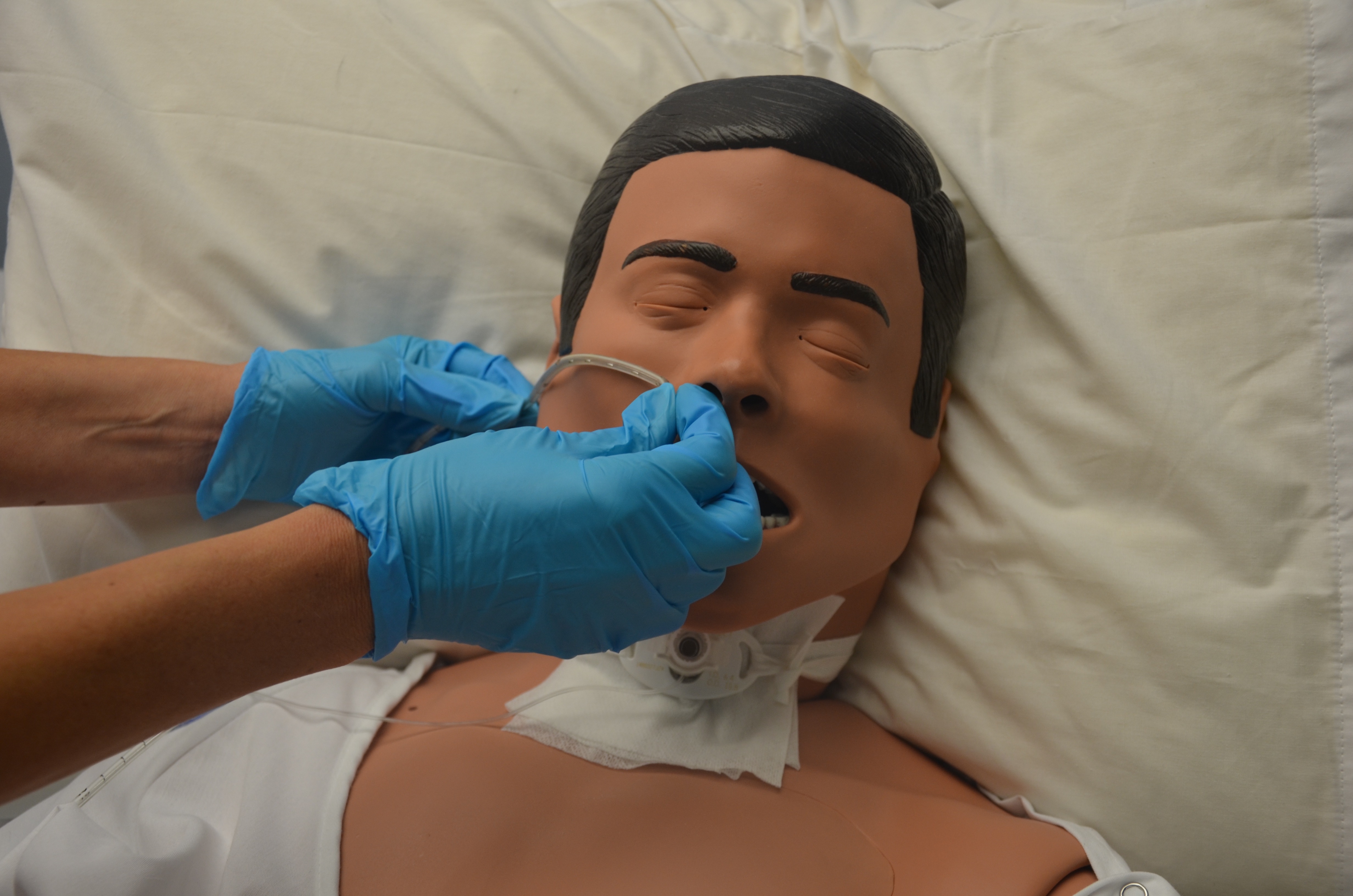
| 15. Have patient drop head forward and breathe through the mouth. | Dropping the head forward closes the trachea and opens the esophagus, which allows the NG tube to pass more easily through the nasopharynx and into the stomach. | ||
| 16. Insert NG tube tip slowly into the patient’s nostril and advance it steadily, in a downward direction, along the bottom of the nasal passage, with the curved end pointing downward in the direction of the ear on the same side as the nostril. | This follows the natural anatomical alignment of the nasopharynx.
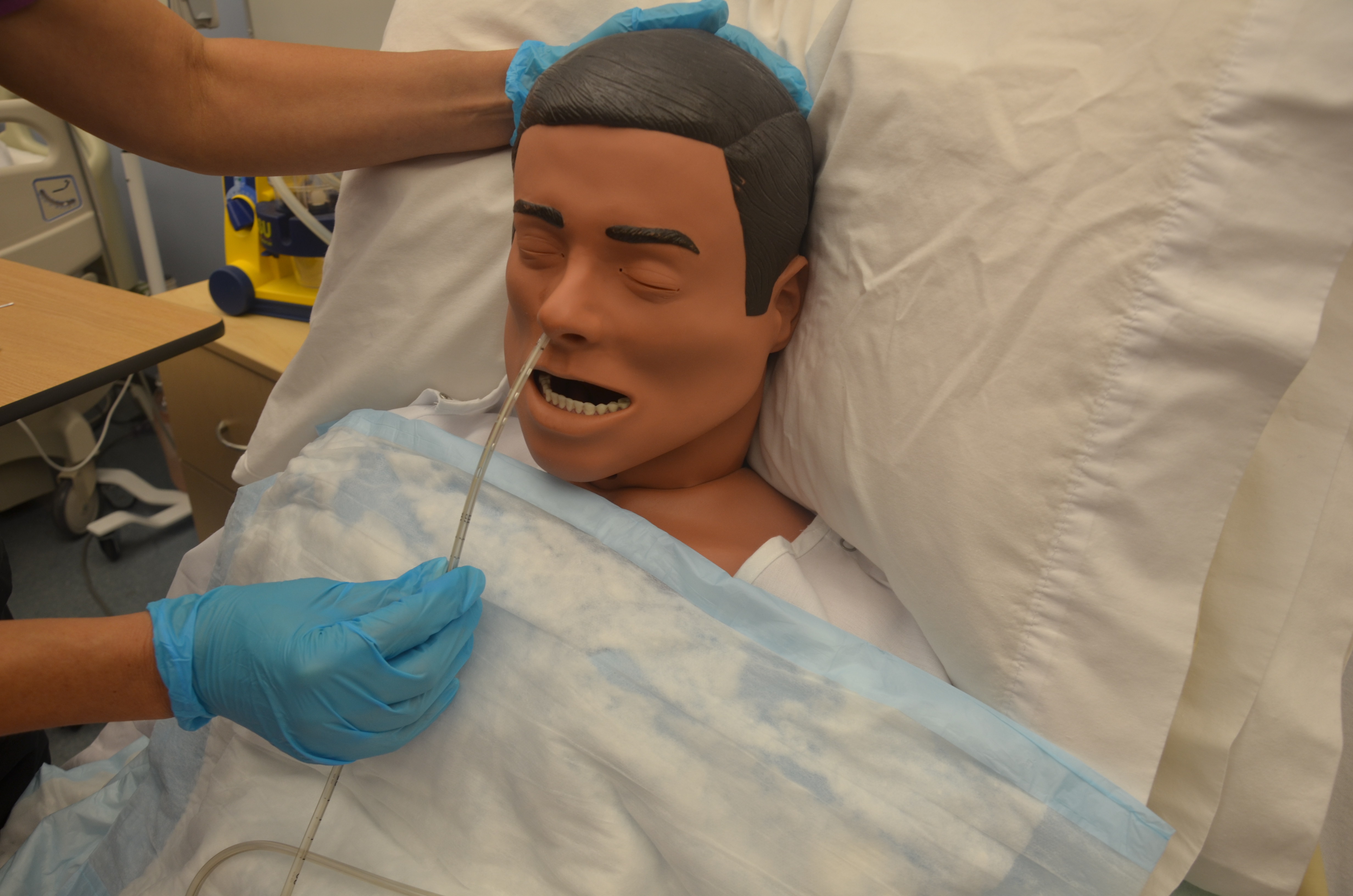 |
||
| 17. You may feel slight resistance as you advance along the nasal passage. Twist the tube slightly, apply downward pressure, and continue trying to advance the tube. If significant resistance is felt, remove the tube and allow the patient to rest before trying again in the other nostril. | It is common for the patient to feel discomfort, and this may be expressed with light coughing and gagging. More aggressive coughing and gagging may indicate that the tube has entered the airways, in which case you should STOP and wait for the coughing to stop. If it doesn’t stop, withdraw the NG tube.
 |
||
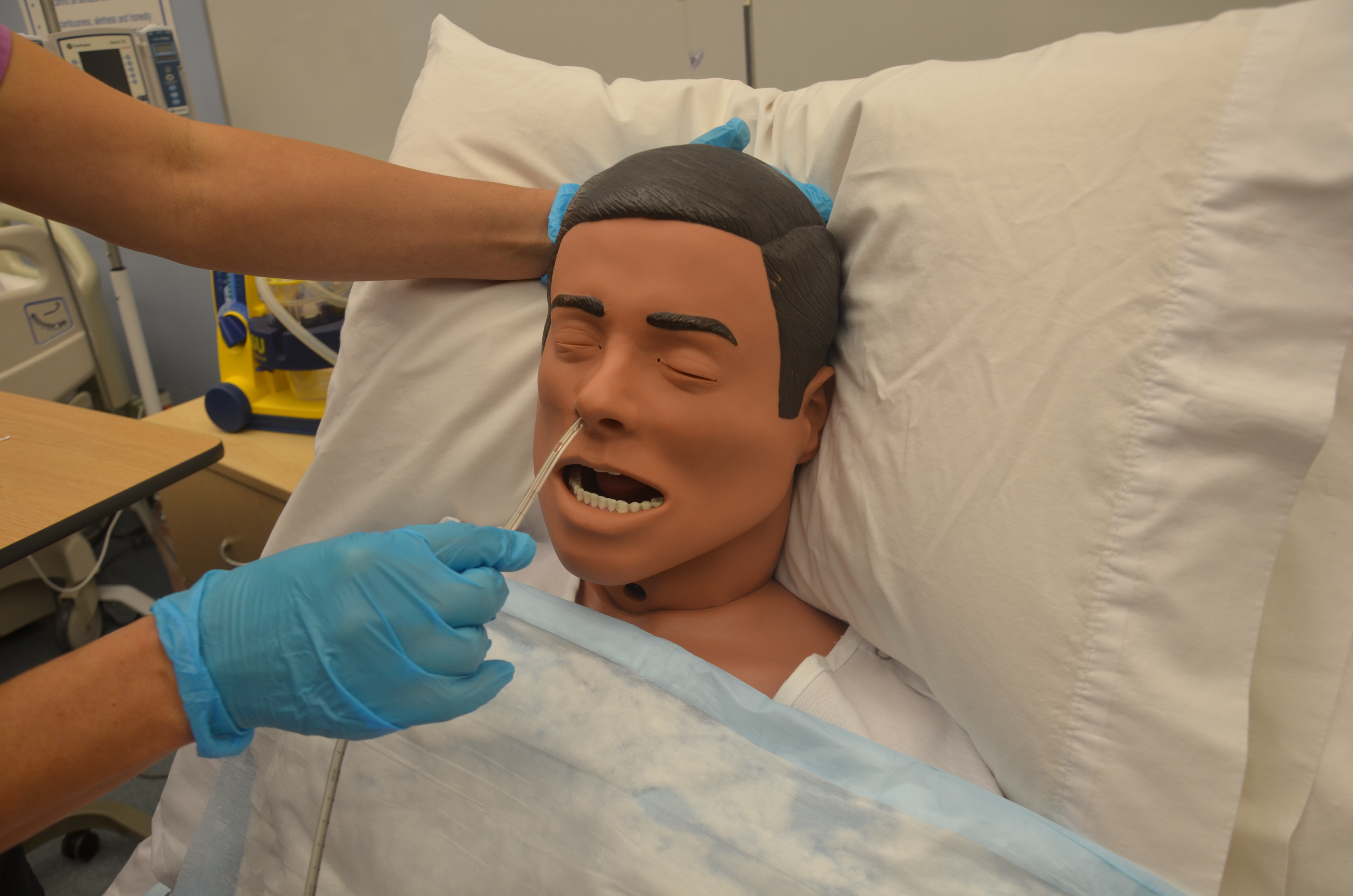
| 18. If the patient has difficulty in passing the NG tube, you may ask the patient to sip water slowly through a straw unless oral fluids are contraindicated. If oral fluids are not allowed, ask the patient to try dry swallowing while you advance the tube. | If patient continues to gag or cough, check that the tube is not coiled in the back of the mouth, using a tongue blade and a flashlight to check the back of the mouth. If tube is coiled, withdraw the tube until only the tip of the tube is seen in the back of the mouth. Then try advancing the tube again while the patient tries to swallow.
 |
||
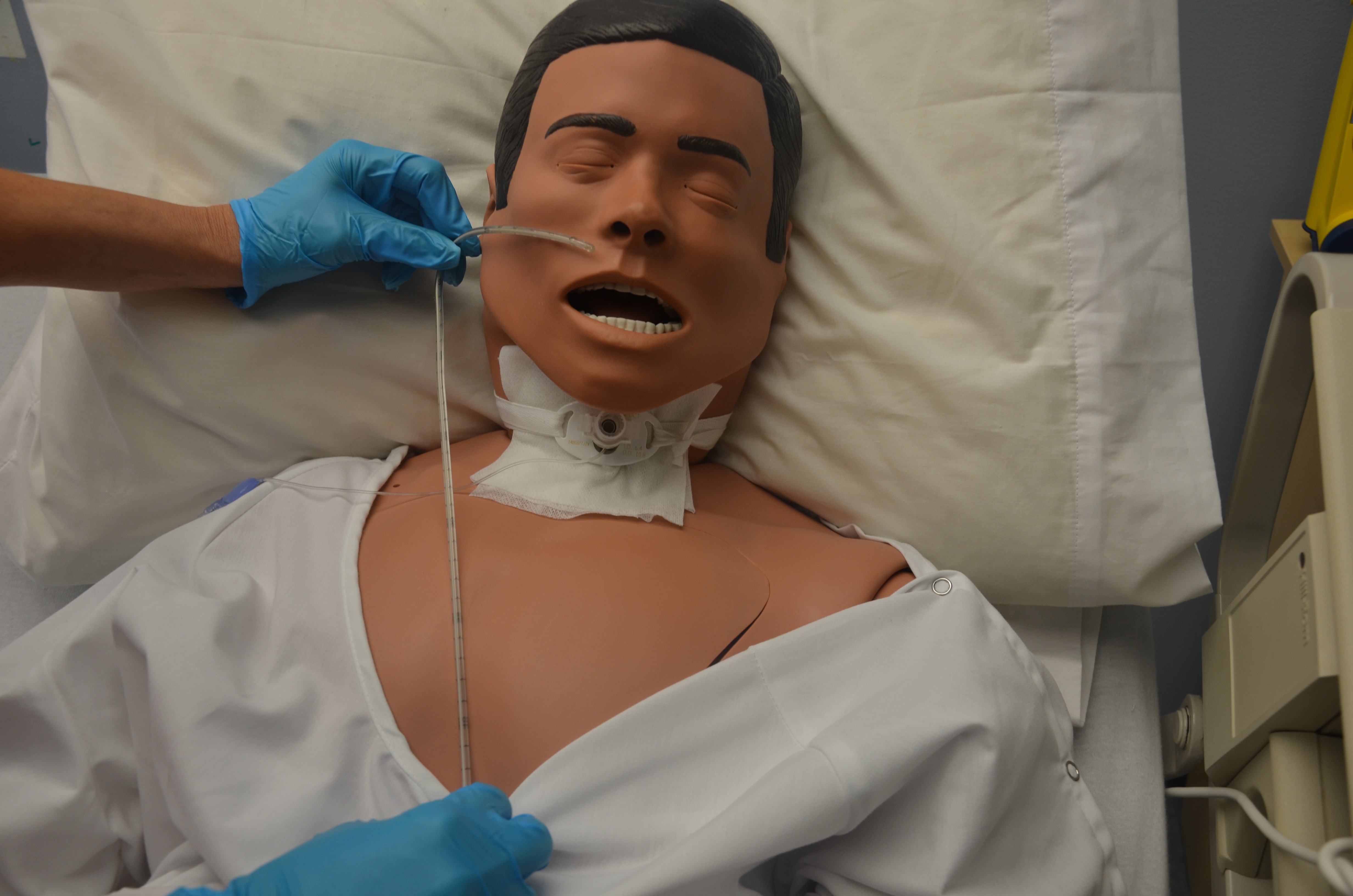
| 19. Continue to advance NG tube until you reach the mark/tape you had placed for measurement. | This ensures accurate placement. | ||
| 20. Temporarily anchor the tube to patient’s cheek with a piece of tape until you can check for correct placement. | This prevents displacement of the NG tube while checking placement.
 |
||
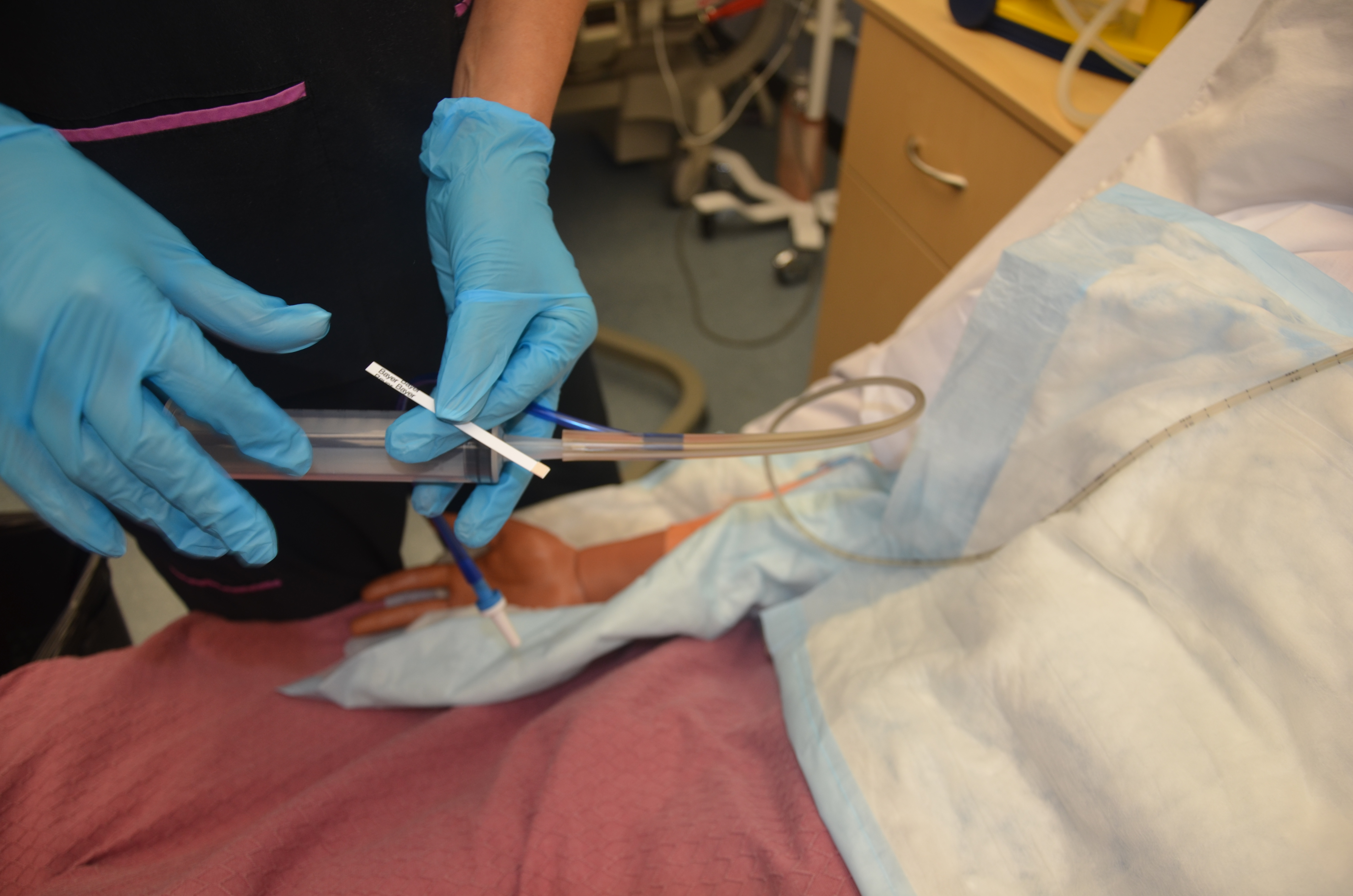
21. Verify tube placement according to agency policy. This may include
Color-coded pH paper is usually used, as an initial and interim check, to confirm that acidic contents are present. Then an X-ray is taken to confirm placement prior to using NG tube for feeding. |
The contents aspirated from the tube should be acidic with a pH < 5. If the pH is more than 6, it may indicate the presence of respiratory fluids or small bowel content, and the tube should be removed. Note: some medications alter gastric pH thus making this method of assessing placement NOT 100% reliable.
 Auscultation of air being injected into the stomach is not a reliable means to determine position of a feeding tube . It cannot distinguish between gastric and small bowel placement nor if the tube tip is in the esophagus. |
||
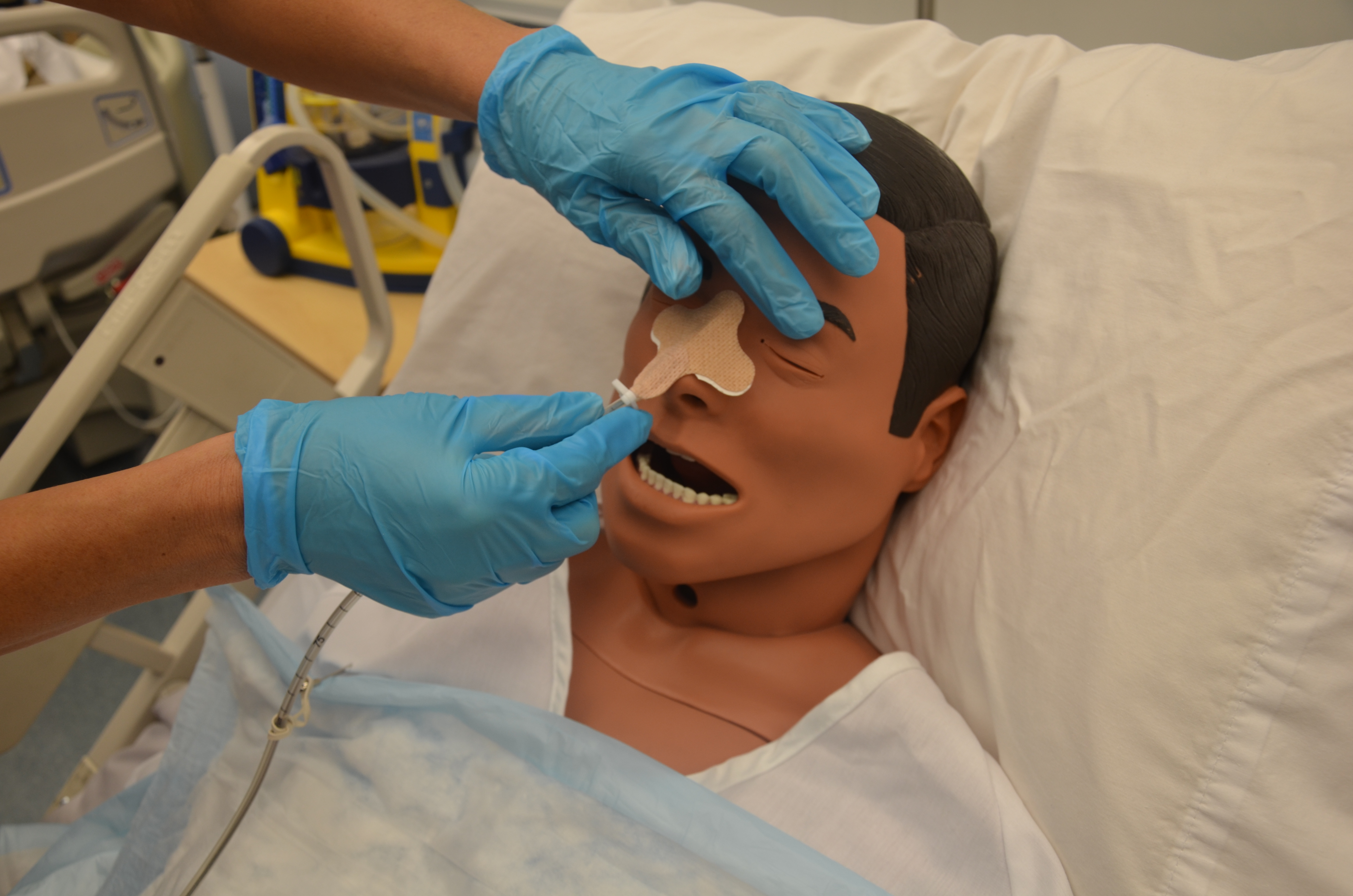
| 22. Once the tube placement has been confirmed, secure the tube to the patient’s nose with tape or a securement device.
Determine external length (the length of tubing extending from the nose to the outer end of the tube). |
This aids in timely recognition and identification of tube displacement or migration. | ||
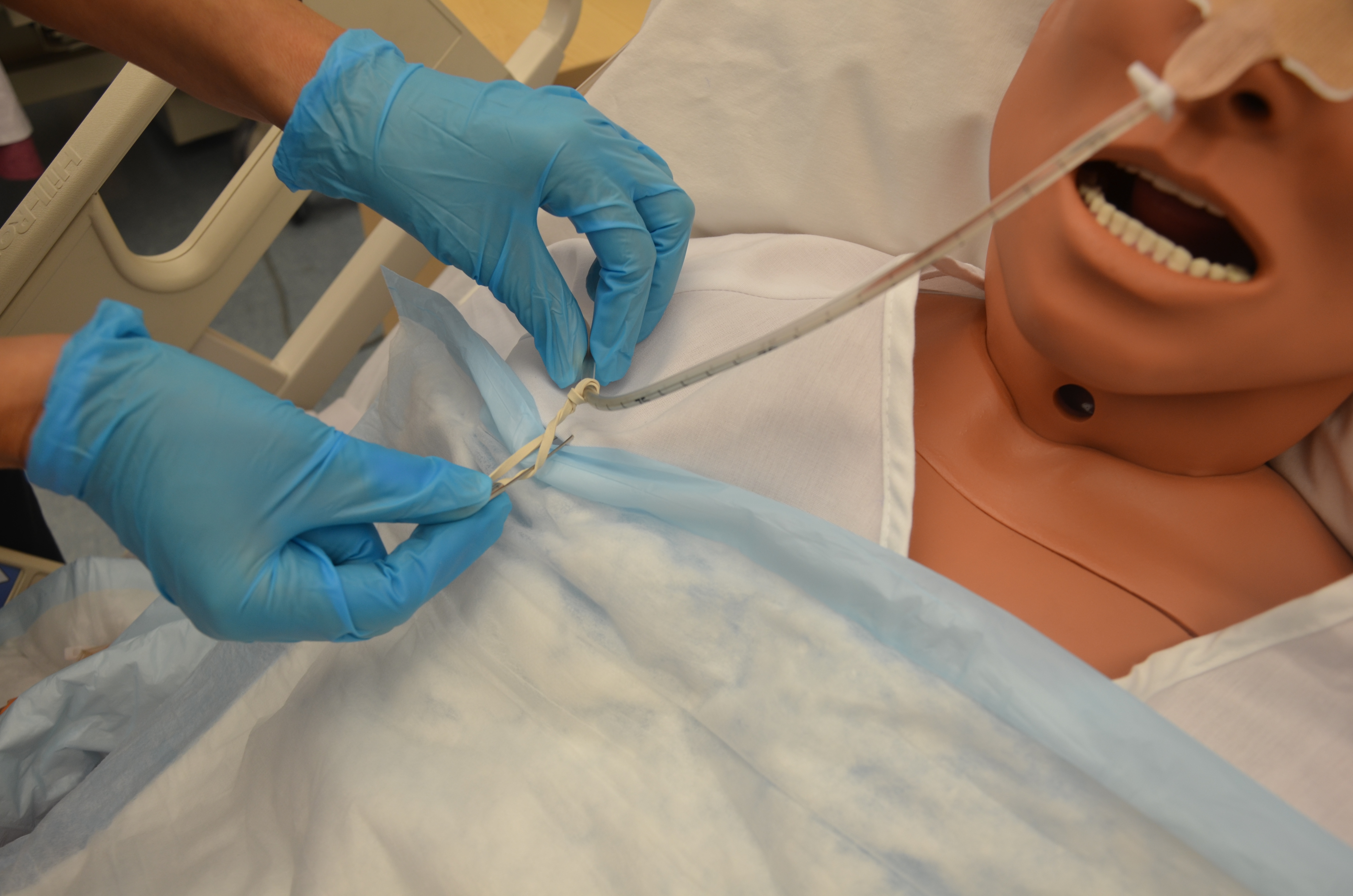
| 23. Secure the tube to the patient’s gown with a safety pin, allowing enough tube length for comfortable head movement.
Help the patient to a comfortable position. |
This keeps the NG tube in place.
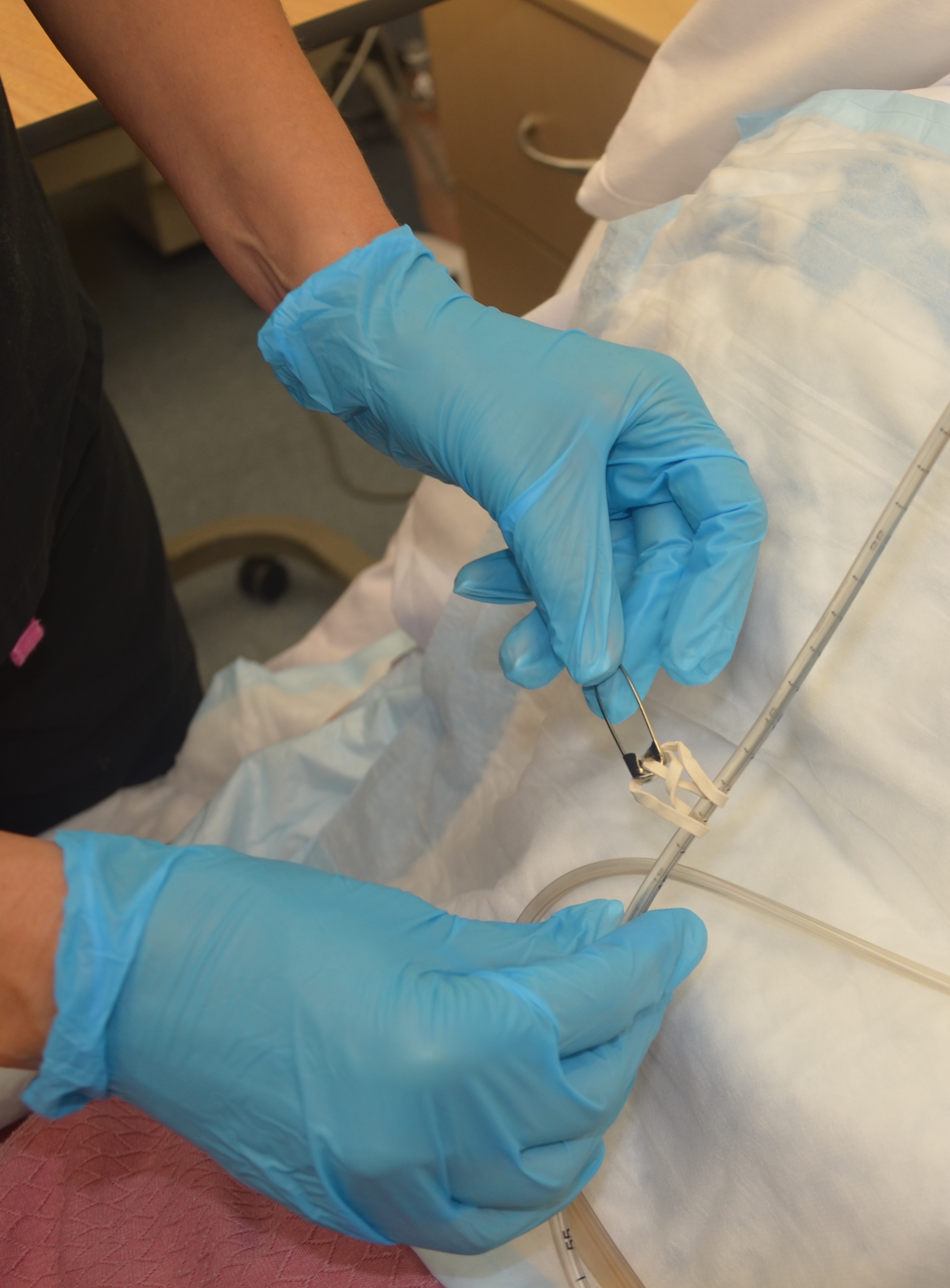 Persons with tube feeds require the head of bed elevated at 30 degrees (or as per agency policy) unless contraindicated to ↓ risk of aspiration. |
||
| 24. Document the procedure according to agency policy, and report any unexpected findings to the appropriate healthcare provider. | Timely and accurate documentation promotes patient safety.
Sample documentation: date / time: Abdomen distended, firm. Reports ++ nausea. Frequent vomiting throughout morning. No bowel sounds. Reported to Dr GI. Orders received. #16 levine inserted right nare for 800 ml dark green returns. Attached to low suction. Tolerated well with reports of less nausea following.——RLeaf RN |
||
| Data sources: BCIT, 2015c; Berman & Snyder, 2016; Bourgault et al., 2014; Potter et al., 2018; Simons & Abdallah, 2012. | |||
Special Considerations with NG Tubes:
- Always assess correct placement of the NG tube prior to infusing any fluids or tube feeds as per agency policy. Check external length, color and pH of the fluid aspirated from the tube. Routine evaluation of tube placement will promote patient safety by reducing risk of aspiration. Do not instill air to test location of tube.
- Do not give the patient anything to eat or drink without knowing that the patient has passed a swallowing assessment.
- If changing the gown or re-positioning the patient, take care not to pull on the NG tube. Remember to unfasten the tube from the gown and refasten the tube afterward.
- If the NG tube falls out of the patient, it is not an emergency. But be sure to assess your patient.
- A patient who appears to be in respiratory distress should be considered an emergency, and emergency procedures should be followed. Respiratory distress may present as coughing, choking, or reduced oxygen saturation.
Removing a NG Tube
A NG tube should be removed if it is no longer required. The process of removal is usually very quick. Prior to removing the NG tube, verify physician orders. If the NG tube is ordered to remove gastric contents, the physician’s order may state to “trial” clamping the tube for a number of hours to see if the patient tolerates oral intake or their own accumulation of gastric secretions prior to the tube removal. During the trial, the patient should not experience any nausea, vomiting, or abdominal distension. If they do experience these things, simply reattach the NG to suction. To review how to remove a NG tube, refer to Checklist 81.
Checklist 81: Removal of a NG TubeDisclaimer: Always review and follow your agency policy regarding this specific skill. |
|||
Safety considerations:
|
|||
Steps |
Additional Information |
||
| 1. Verify healthcare provider’s orders to remove NG tube. | An order is required to remove an NG tube. | ||
| 2. Collect supplies. | Supplies include waterproof pads, 20 ml catheter tip syringe, tissues, non-sterile gloves, and plastic garbage bag. | ||
| 3. Verify patient using two identifiers. Explain procedure to patient and place patient in high Fowler’s position. | Follow agency policy for proper patient identification. | ||
| 4. Perform hand hygiene. Place waterproof pad on patient’s chest. | This reduces the transmission of microorganisms.
 |
||
5. Depending on the purpose of the tube either:
|
This reduces risk of aspiration of tube feed and makes disposal of equipment easier.
 |
||
| 6.Flush tube with air and then kink tube |
 Flushing the tube with air and kinking prevents leakage of fluid from the tube and prevents aspiration of tube feed or residual gastric secretions. |
||
| 7. Unclip NG tube from patient’s gown. | This allows for tube to be easily removed and disposed of immediately.
 |
||
| 8. Remove securement device from nose (this is the last step prior to removing the tube thus preventing accidental tube removal before either the nurse or client are ready) | 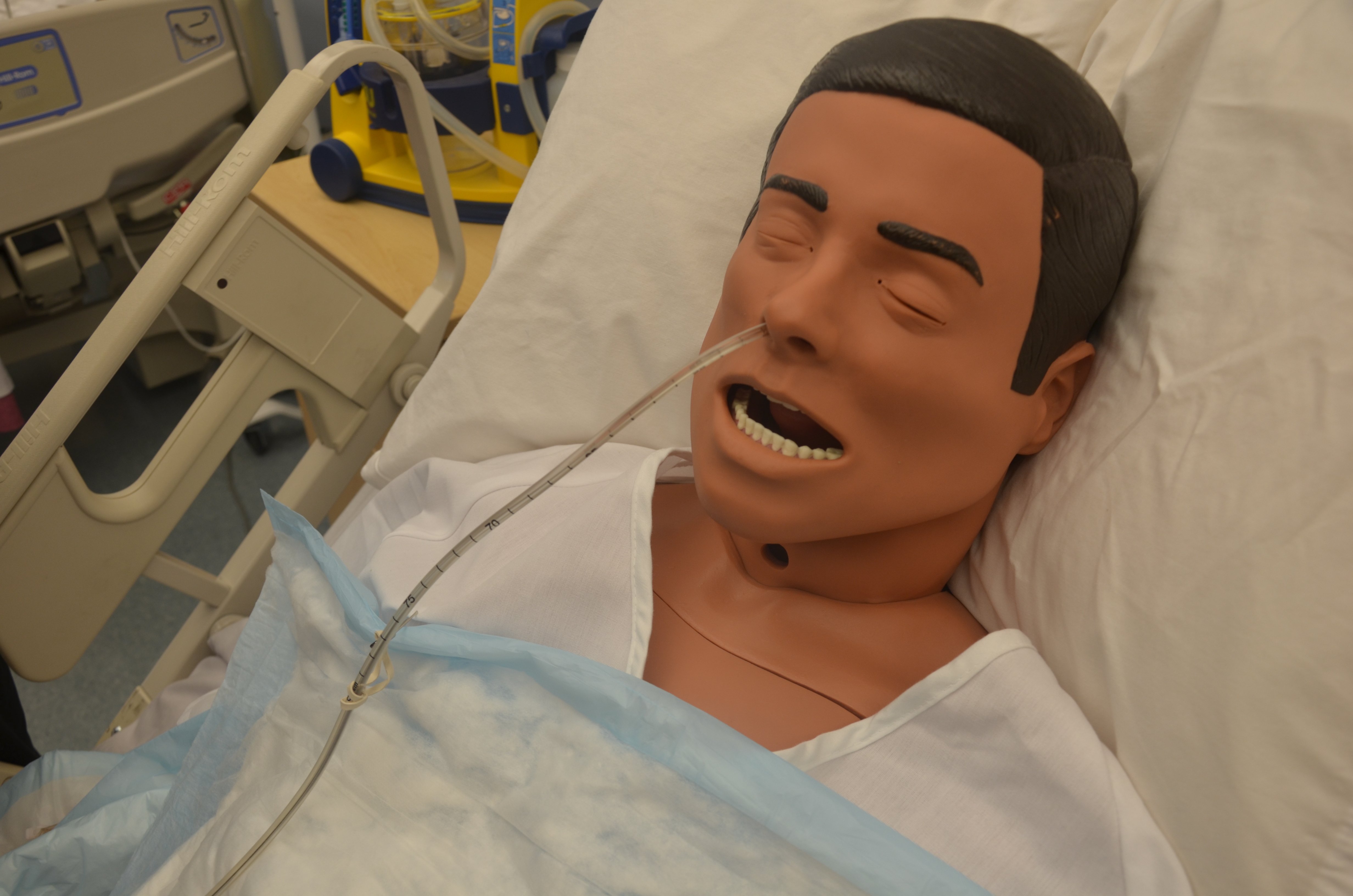 |
||
| 9.Instruct patient to take a deep breath and hold it. | Holding the breath closes the glottis, decreases risk of aspiration, and distracts the patient. | ||
| 10. Hold the NG tube near the naris and gently pull out tube in a swift, steady motion. Dispose of tube in garbage bag. |
  |
||
| 11. Offer tissue or clean the nares for the patient, and offer mouth care as required. | This clears the nares/nasal passages of any remaining secretions.
|
||
| 12. Remove gloves and place patient in a comfortable position. Assess patient’s level of comfort. Perform hand hygiene. | This promotes patient comfort and reduces the transmission of microorganisms. | ||
| 13. Document procedure according to agency policy | Document removal of NG tube and patient response to the removal. | ||
| Data source: BCIT, 2015b; Perry et al., 2018 | |||
Critical Thinking Exercises
- You are inserting a nasogastric tube and the patient begins to cough and turn red in the face. Explain your next steps.
- Your patient has a nasogastric tube and is requesting water because her throat feels dry. Describe your next actions.
- Your patient calls you to say they’ve accidentally pulled out the NG. Explain your next steps.
