Chapter 2. Patient Assessment
2.6 Head-to-Toe Assessment: head and neck / Neurological Assessment
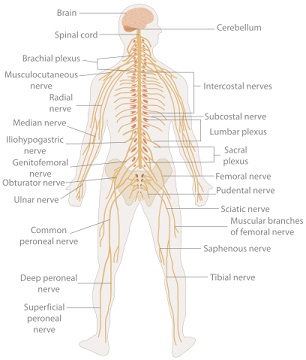
The neurological system is responsible for all human function. It exerts unconscious control over basic body functions, and it also enables complex interactions with others and the environment (Stephen, Skillen, Day, & Jensen, 2012). A neurological assessment begins when the nurse first interacts with the client and involves observations about appearance, communication patterns, and general behaviour. The first part of the checklist provides a general overview of performing a basic neurological assessment. In some situations a more focused neurological assessment is necessary. The last part of the checklist provides some guidelines for some elements of a focused neurological assessment.
Checklist 16 provides a guide for subjective and objective data collection in a neurological assessment.
Objective DataConsider the following observations.
|
|
Steps |
Additional Information |
General appearance
 |
Observations about general appearance may provide insight into other physical or psychosocial issues affecting the patient.
If appearance is unkempt, it may suggest that the patient struggles with achieving activities of daily living. The nurse would further their questioning to elicit greater understanding, and potentially to refer to other healthcare professionals subsequently.
|
| Level of consciousness (LOC)
|
Altered LOC may indicate substance use, fatigue, brain injury, neurological disorder, mania, or depression. |
| Inspect eyes & nose for drainage.
|
Drainage from eyes or nose may indicate infection, allergy, or injury. |
| Note nature of eye contact during interview.
|
The extent of eye contact may reflect cultural norms, individual way of being, or possibly mental health issues. |
| Glasses, contacts, hearing aids
|
People who need these devices but don’t have them, or if the devices are not in working order, may experience some level of isolation because of difficulty interacting with the world around them. |
Inspect for facial asymmetry.
 |
Facial asymmetry may indicate neurological impairment or injury. Unusual findings should be followed up with a focused neurological system assessment. |
| Evidence of nasal trauma. Ability to breathe through nose.
|
Nasal flaring or use of accessory muscles when breathing may indicate altered breathing patterns. Unusual findings should be followed-up with a focused respiratory assessment. |
| Inspect mouth, tongue, and teeth for moisture, colour, dentures, hygiene.
|
Dry mucous membranes may indicated altered hydration. Dental disease can influence one’s general health. |
| Ability to swallow
|
Difficulty swallowing may suggest neurological impairment. Frequent coughing or choking associated with eating or drinking may suggest risk of aspiration. Unusual finding should be followed-up with a swallow assessment and a referral to an occupational therapist. |
| Neck range of motion (ROM)
|
This includes flexion, extension (front and back, and side to side) and ability to rotate the neck side to side.
Impaired neck ROM may indicate an old injury. Neck pain and stiffness (nuchal rigidity) may be related to old injury or signs and symptoms of a serious neurological illness. |
| Ability to communicate
|
Difficulty communicating may be the result of a language barrier or neurological impairment. Communication barriers related to language differences between the patient and healthcare givers might be alleviated through interpreters making information available in the patient’s language.
Communication barriers related to neurological impairment require further investigation and a creative approach during patient care. |
General arm and leg strength.
   |
General arm and hand strength can be assessed by asking the patient to extend their arms and grip the nurse’s hands simultaneously. General leg strength can be assessed by asking the patient to dorsiflex, plantar flex, and bend each knee. Dorsiflexion strength can be assessed by asking the patient to pull up on their feet while the nurse applies some resistance to the top of the feet. Plantar flexion strength is assessed while the nurse applies some resistance to the bottom of the feet while asking the patient to push (i.e., step on the gas). Always compare extremities. |
Subjective DataAsk about vision, hearing, headaches, neck stiffness, history of head injury, neurological disease, history of seizures, stroke, memory loss, mental health history. |
|||||||||||||||||||||||||||||||||||||
Focused neuro assessment may also include: |
|||||||||||||||||||||||||||||||||||||
| Pain Assessment | See Chapter 2.42 Pain Assessment | ||||||||||||||||||||||||||||||||||||
| Mental Status Exam (MSE): Is used in psychiatry to guide the examiner to collect data and form impressions about an individual’s mental health. | MSE involves the following components:
For more resources about MSE, go to RNAO’s Nursing Best Practice Guidelines: Outline of a Mental Status Examination. |
||||||||||||||||||||||||||||||||||||
| Mini-Mental State Exam (MMSE): Used to measure cognitive impairment and often performed in the context of persons with dementia. | For more information about the MMSE see BCGuidelines.ca (2014) Standardized Mini-Mental State Exam (SMMSE) | ||||||||||||||||||||||||||||||||||||
Glasgow Coma Scale (GCS): Used to guide assessment in patients with head injury, suspected brain bleeds, stroke, and cranial surgery, and in persons with altered level of consciousness. In general, the GSC measures assess:
The lower the score, the more serious the neurological impairment. This assessment tool allows for objective assessment and greater reliability in terms of being able to observe patterns and trends in the patient’s health status. |
Glasgow Coma Scale (adapted from Jarvis et al., 2014, p. 699)
For more information about neuro assessment go to Critical Care Services Ontario’s Guidelines for Basic Adult Neurological Observation. |
||||||||||||||||||||||||||||||||||||
| Assess arm drift by asking the patient to extend their arms in front of them and close their eyes. | Drift of one arm may suggest neurological dysfunction. Report concerns immediately. | ||||||||||||||||||||||||||||||||||||
| Pupil Assessment: Assess pupils for size, equality, reaction to light, and consensual reaction to light.
|
In a darkened room ask the patient to look at your nose. With a lit flashlight, shine the light moving from the lateral across the open eye to the space between the eyes. Note the pupil’s reaction to light.
Repeat on the other side. To test consensual reaction, have the patient look at your nose. Shine a flashlight from the hairline at the mid-forehead to the space between the eyes. Observe for the pupils to react equally at the same time. Pupils that are equal and reactive to light are described as PERL. Alterations may be a part of the patient’s norm or they may indicate severe neurological dysfunction, and should be reported immediately. |
||||||||||||||||||||||||||||||||||||
| Dermatome Assessment: Dermatomes are areas of skin supplied by a single spinal nerve.
To perform a dermatome assessment use ice. Begin at the neck area. Move the ice downward along the side of the patient’s body asking them to indicate if and when sensation changes. Continue to the lateral side of the foot. Repeat on the other side. 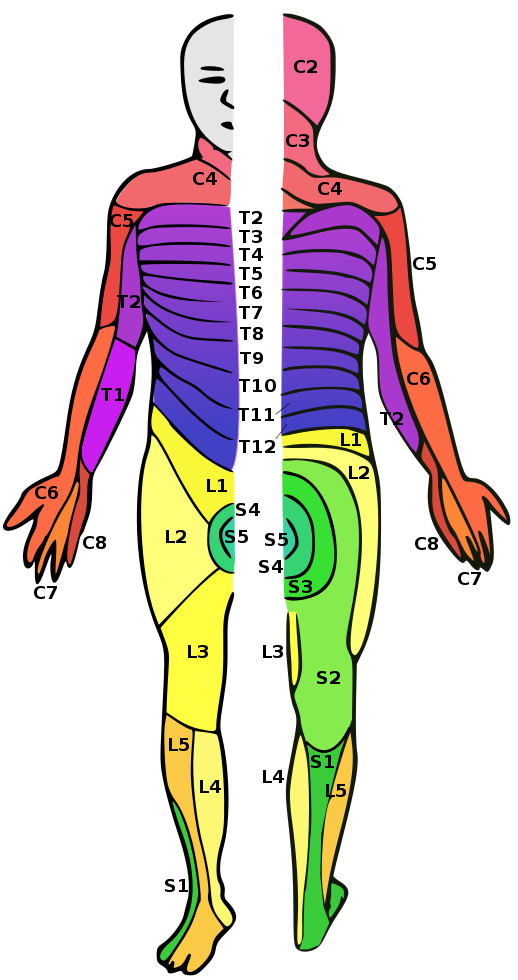 |
Dermatome assessment may be indicated in persons with spinal cord injury or when patients receive spinal or epidural analgesics (local anesthetics).
Depending on the context, changes in dermatome levels may indicate local anesthetic is moving up or down in the epidural space. In spinal cord injury, alterations in dermatomes may indicate improving or worsening changes in patient status. Document blocked dermatomes according to agency guidelines. E.g., Right side: T12-L1; Left side: L1-L4. |
||||||||||||||||||||||||||||||||||||
| Sedation Score Assessment: Nursing assessment of opioid induced sedation is quick and easy. Having a guide provides some level of consistency between assessors and provides important information to the healthcare team about trends in the patient’s level of sedation. | Sample Sedation Score Assessment (adapted from Pasero, 2009)
Sedation scores may form a part of an agency’s assessment protocol(s). Some agencies provide direction for opioid use based on the sedation score. |
||||||||||||||||||||||||||||||||||||
| The National Institute of Health Stroke Scale (NIHSS): Used specifically when stroke is suspected. It is often a part of an institution’s stroke protocol. | For reference see:
Heart and Stroke Foundation. (2019). Canadian partnership for stroke recovery. Retrieved from https://www.stroke.nih.gov/documents/NIH_Stroke_Scale_508C.pdf. |
||||||||||||||||||||||||||||||||||||
Potential neurological related nursing diagnoses:
|
|||||||||||||||||||||||||||||||||||||
| Data sources: Alberta Health Services, 2009; Assessment Skill Checklists, 2014; Critical Care Services Ontario, 2014; Heart and Stroke Foundation, 2019; Jarvis, Browne, MacDonald-Jenkins, & Luctkar-Flude, 2014; Pasero, 2009; Perry, Potter, & Ostendorf, 2018; RCH, 2015; RNAO, n.d.; Stephen et al., 2012; Wilson & Giddens, 2013 | |||||||||||||||||||||||||||||||||||||

Critical Thinking Exercises
- What patient situations would require a dermatome assessment?
- When caring for a client post CVA, consider the difference between completing a Glasgow Coma Scale (GCS) assessment and a National Institutes of Health Stroke Scale (NIHSS).
- Besides opioid induced sedation, identify one other situation where sedation score might be appropriate part of an assessment.
Attributions:
Figure 2.4 Neurological System by the Emirr is used under a CC BY 3.0 license.
Figure 2.5 A Man’s Face by Christiaan Brigs is used under a CC BY-SA 3.0 license.
Figure 2.6 Bells Palsy by CDC and United States Department of Health and Human Services is in the public domain.
Figure 2.8 A Diagram Showing Human Dermatomes by Ralf Stephanis in the public domain.

{kind=link}
{kind=link}
{kind=link}
{kind=link}