Chapter 8. Intravenous Therapy
8.3 Types of Venous Access
Safe and reliable venous access for infusions is a critical component of patient care in acute and community health settings. There are a variety of options available, and a venous access device must be selected based on the duration of IV therapy, type of medication or solution to be infused, and the needs of the patient. In practice it is important to understand the options of appropriate devices available.
This section will describe two types of venous access: peripheral IV access and central venous catheters. Besides observing the site for complications, accessing, flushing, and removal of IVADs, tunneled catheters, and catheters used for hemodialysis require specialized skill and they are not within the scope of this textbook.
Peripheral Venous Access Device—Short Cannula (PVAD-Short) a.k.a. Short Peripheral Catheter (SPC)
A PVAD-short cannula is a common, preferred method for short-term IV therapy in the hospital setting (see Figure 8.1). Principles of asepsis are followed during insertion. Sites are covered with dressings, which can be a sterile transparent semi-permeable dressing or a gauze dressing if the site is bleeding (RNAO, 2005/2008). Dressings serve to keep the site sterile and prevent accidental dislodgement (CDC, 2017). Upper extremities (hands and arms) are the preferred sites for insertion by a specially trained healthcare provider. If a lower extremity is used, remove the peripheral IV and re-site in the upper extremities as soon as possible (CDC, 2017; McCallum & Higgins, 2012). The hub of a short intravenous catheter should be attached to IV extension tubing with a needleless cap (Fraser Health Authority, 2014).
PVAD-shorts are used for infusions under six days and for solutions that are iso-osmotic or near iso-osmotic (CDC, 2017). They are easy to monitor and can be inserted at the bedside. CDC (2017) recommends that PVAD-shorts be replaced every 72 to 96 hours to prevent infection and phlebitis in adults. Other literature suggests that PVAD-short catheters be changed based on individual assessment of the site and not specific time frames (Gorski et al., 2012). Many agencies require additional training to initiate IV therapy, but the care and preparation of equipment, and the maintenance of an IV system, is the responsibility of the trained healthcare provider.


PVAD-short sites are prone to phlebitis and infection, and should be removed (CDC, 2017) as follows:
- Every 72 to 96 hours and p.r.n. Some literature challenges this firm timeline and suggests that sites should be assessed individually for decisions about removal (Gorski et al., 2012).
- As soon as the patient is stable and no longer requires IV fluid therapy
- As soon as the patient is stable following insertion of a cannula in an area of flexion
- Immediately if tenderness, swelling, redness, or purulent drainage occurs at the insertion site
- When the administration set is changed (IV tubing)
Midline Catheters
A midline catheter differs from a PVAD-short catheter in terms of length. Midline catheters are 7.5 to 20 cm long; usually inserted into an antecubital fossa; the catheter tip sits in the vein below the level of the axilla. They are considered for IV therapy longer than a PVAD-short although the literature is inconsistent in terms of how long. The range is from 6 days to 8 weeks (RNAO, 2005/2008). While the tip of the catheter sits in a vessel larger than a peripheral vein, it is significantly smaller than the superior vena cava (SVC). As such the types of drugs and solutions that can be safely administered through a midline catheter are the same as a PVAD-short (Rosenthal, 2007).

Peripherally inserted central catheters (PICCs) are also inserted peripherally, but because the tip of the catheter sits in the superior vena cava, PICCs will be discussed with CVADs.
Central Venous Access Device (CVAD)
A CVAD is a type of catheter or device inserted into the central circulation. They are also referred to as a central venous catheter (CVC) or central line (see Table 8.5). Usually the tip of the catheter terminates in the superior vena cava just above the right atrium. For CVADs that are inserted femorally, the tip of the catheter should sit in the inferior vena cava. Because of the large size of vein and the high volume blood flow associated with it, a CVAD has many advantages over a PVAD-short. This includes the ability to deliver fluids and/or medications that can be overly irritating (high or low pH, high osmolality) to small peripheral veins; the ability to access multiple lumens and deliver multiple medications or solutions simultaneously even if they are incompatible with each other (Fraser Health Authority, 2014); the ability to deliver large volumes quickly; and the ability to maintain IV access over a prolonged period of time (Perry et al., 2018). Some CVADs have technology associated with them that allows for monitoring of central venous pressure, which is beyond the scope of this textbook.
While PVAD-short catheters are generally removed within a few days, CVADs can remain in situ much longer (Perry et al., 2018):
- Non-tunneled percutaneous CVADs for several days to weeks.
- IVADs can remain in place and function for many years.
- PICCs can remain in place as long as there is no evidence of complications.
CVADs can be inserted on the unit or in the operating room through the jugular, subclavian, or femoral veins, or via the chest or upper arm peripheral veins (Perry et al., 2014). Femoral veins are not recommended, as the rate of infection is increased in adults (CDC, 2017; Safer Healthcare Now, 2012). Initial access of a CVAD should only be done after placement is verified. Sometimes this includes a chest x-ray. Equipment used during PICC insertion has the capability to confirm placement through ultrasound technology (Safer Healthcare Now, 2012; Interior Health, 2012). Using an IV pump will reduce risk of some complications associated with CVADs and may be part of your agency policy. Some CVADs can be removed by a nurse with specific training (PICC, percutaneous non hemodialysis line), others must be removed surgically (tunneled catheter, IVAD).
Table 8.5 Types of Central Venous Catheters (CVCs)Safety considerations:
|
||
| Percutaneuos central venous catheter (CVC)—non hemodialysis | Tip location: The tip of the catheter is located in the superior vena cava (SVC).
Can be inserted at the bedside by specially trained physician or nurse. The percutaneous CVAD is inserted directly through the skin. The internal or external jugular, subclavian, or femoral vein is used. Most commonly used in critically ill patients. Can be used for days to weeks. Usually held in place with sutures or a manufactured securement device.   |
|
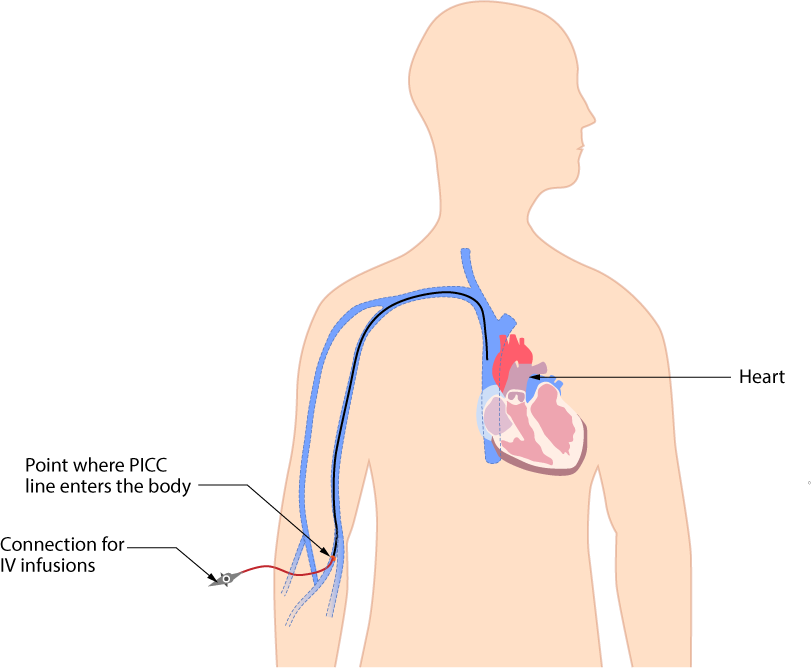
| Peripherally inserted central catheter (PICC) | Tip location: The tip of a PICC is located in the SVC.
A PICC (see Figure 8.4) may be inserted at the bedside, in a home, or in the radiology setting. The line is inserted through the antecubital fossa or upper arm (basilic or cephalic vein) and is threaded the full length until the tip reaches the SVC. Can provide venous access for up to one year. The patient may go home with a PICC. PICCs can easily occlude and may not be used with dilantin IV. It is held in place with sutures or a manufactured securement device for as long as there is no evidence of complications.
  |
|
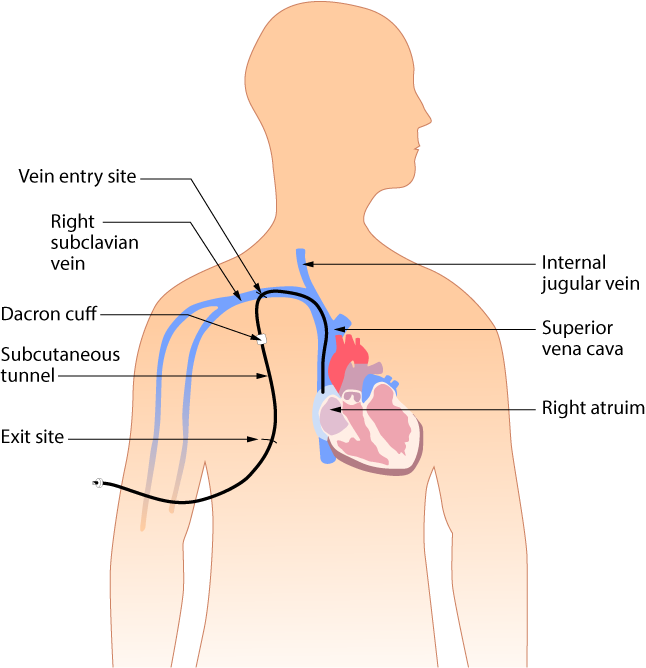
| Tunnelled central venous catheter | A tunnelled CVC, also known as a Hickman, Broviac, or Groshong, is a long-term CVC . The catheter tip is in the superior vena cava. Insertion is a surgical procedure, in which the catheter is tunnelled subcutaneously under the skin in the chest area before it enters the SVC. A tunnelled catheter may remain inserted for months to years. These CVCs have a low infection rate due to a Dacron cuff, an antimicrobial cuff surrounding the catheter near the entry site, which is coated in antimicrobial solution and holds the catheter in place after two to three weeks of insertion.
  |
|
Implanted venous access device (IVAD)
|
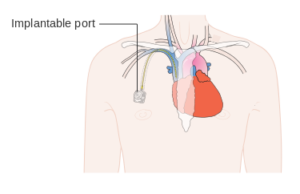
The implanted central venous access device (IVAD) (a.k.a. implanted central venous access catheter, ICVC) is inserted into a vessel, body cavity, or organ, and is attached to a reservoir or “port” located under the skin. The ICVC is also referred to as a port a catheter or port a cath. A surgical procedure is required to insert the device, which is considered permanent. The device may be placed in the chest, abdomen, or inner aspect of the forearms. For some this is preferred because of body image. For others this is preferred because the unit is concealed under the skin, so it is ideal for those who like to swim or use a hot tub. IVADs are accessed by specially trained personnel using a non-coring needle.
  |
|
| Data sources: Fulcher & Frazier, 2011; Perry et al., 2018 | ||
CVCs have specific protocols for accessing, flushing, disconnecting, and assessment. All healthcare providers require specialized training to care for, manage complications related to, and maintain CVCs as per agency policy. Never access or use a central line for IV therapy unless trained as per agency policy. For more information on CVC care and maintenance, see the suggested online reference list at the end of this chapter.
Healthcare providers should assess a patient with a central line at the beginning and the end of every shift, and as needed. For example, if the central line has been compromised (pulled or kinked), ensure it is functioning correctly. Each assessment should include:
- Type of CVC and insertion date: Reason for CVC?
- Dressing: Is it dry and intact?
- Lines: Secure with stat-lock, sutures, or Steri-Strips?
- Review: Patient still requires a CVC?
- Insertion site: Free from redness, pain, swelling?
- Positive pressure cap: Attached securely?
- IV fluids: Running through an IV pump?
- Lumens: Number of lumens and type of fluids running through each?
- Vital signs: Fever?
- Respiratory/cardiovascular check: Any signs and symptoms of fluid overload?
Central Venous Catheter Structure and Technology
Understanding central venous catheter structure and technology is necessary for understanding the care and maintenance associated with them. CVADs have specific protocols for accessing, flushing, disconnecting, and assessment. Some agencies require specialized training to care for, manage complications related to, and maintain CVADs. As such, know your agency policy.
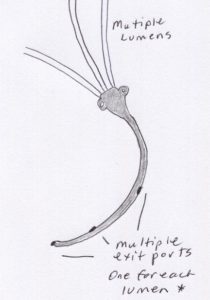
Mulitlumen CVCs
Multilumen catheters allow the infusion of multiple medications and multiple solutions simultaneously because the exit ports are located in different locations along the catheter lumen(s). Medications do not come in contact with each other until they enter the blood stream where turbulent flow and blood volume allow for dilution. When a CVC has more than one lumen, each lumen must be treated as a separate catheter. Thus each lumen receives individual attention in relation to care and maintenance.

Valve Technology: Open-Ended Versus Closed-Ended Lumens
CVCs are available with open and closed ends. Figure 8.11 explains the theory behind valve technology. Table 8.6 outlines some key differences between open versus closed-ended lumens. It is important for the nurse to differentiate them because care and maintenance differs slightly. Recent literature has found limited evidence comparing valved and non-valved PICCs in the incidence of occlusion of the catheters or PICC-related blood stream infection and complications (obstruction, rupture) (Ho & Spry, 2017). Ongoing research will continue to influence nursing practices and as such life long learning is a part of nursing practice.
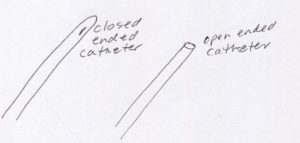
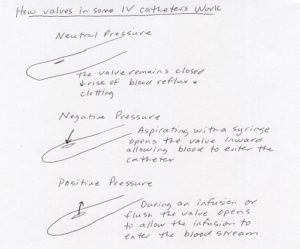
Table 8.6 Characteristics of Open- Versus Closed-Ended CVC Lumens |
|
Open–Ended |
Closed–Ended |
|
|
| Data sources: Perry et al., 2018; RNAO, 2005/2008 | |
Critical Thinking Exercises
- Differentiate different venous access devices: PVAD-short, midline catheter, peripherally inserted central catheter (PICC), percutaneous non hemodialysis central catheter, implanted venous access device (IVAD), and tunneled catheter. Provide one indication for each.
- Identify a situation where having a multilumen CVC is desired.
Attribution
Figure 8.1. Intravenous therapy is from Michaelberry at English Wikipedia and is used under a CC BY 3.0 Unported license.
Figure 8.2. Midline catheter is from BruceBlaus and is used under a CC BY-SA 4.0 international license.
Figure 8.3. Percutaneous CVAD from BCIT (adapted) is used under a CC BY-SA 4.0 international license.
Figure 8.4. Triple lumen is from Jsnop and is in the public domain.
Figure 8.5. PICC from BruceBlaus is used under a CC BY-SA 4.0 international license.
Figure 8.6. Omläggning av PICC [Conversion of PICC] by Nurseirie is used under a CC BY-SA 3.0 unported license.
Figure 8.7 Central Venous Access Device (tunneled) by BruceBlaus is used under a CC BY-SA 4.0 international license.
Figure 8.8. Hickman line catheter with 2 lumens by General Ludd is used under a CC BY-SA 3.0 unported license.
Figure 8.9. Diagram showing an implantable port by Cancer Research UK is used under a CC BY-SA 4.0 international license.
Figure 8.10. Port catheter [cropped from original photo RecurrentbreastCA.gif] derivative by Una Smith is in the public domain.
Figure 8.11. Multiple lumens from author is licensed under a CC BY-SA 4.0 international license.
Figure 8.12. Triple lumen is from author is licensed under a CC BY-SA 4.0 international license.
Figure 8.13. Open ended versus closed ended catheters by author is licensed under a CC BY-SA 4.0 international license.
Figure 8.14. Valve technology – some CVCs is adapted from Registered Nurses’ Association of Ontario. (2005). Care and Maintenance to Reduce Vascular Access Complications. Toronto, Canada: Registered Nurses’ Association of Ontario. Appendix E: Groshong® Valve Function [Image]. p. 69.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Omläggning av PICC [Conversion of PICC]](https://commons.wikimedia.org/wiki/File:PICC_oml%C3%A4ggning.jpg){kind=link}
.png){kind=link}
{kind=link}
{kind=link}
{kind=link}