Chapter 6. Non-Parenteral Medication Administration
6.3 Administering Medications by Mouth and Gastric Tube
Administering Medication by Mouth

Medication is usually given orally, which is generally the most comfortable and convenient route for the patient. Medication given orally has a slower onset and a more prolonged, but less potent, effect than medication administered by other routes (Lynn, 2011). Prior to oral administration of medications, ensure that the patient has no contraindications to receiving oral medication, is able to swallow, and is not on gastric suction. If the patient is having difficulty swallowing (dysphagia), some tablets may be crushed using a clean mortar and pestle or pill crusher. Verify that a tablet may be crushed by consulting a drug reference or a pharmacist.
Medications such as enteric-coated (EC) tablets, capsules, and sustained-release (SR) or long-acting (LA) drugs should never be crushed because doing so will affect the intended action of the medication (Lilley et al., 2016). EC medications are designed to be absorbed in the small bowel. Crushing it would cause absorption in the stomach, potentially causing adverse events. SR and LA medications if crushed would result in high doses being absorbed quickly potentially causing adverse events—some of which could be fatal. If medications are able to be crushed and must be in order to allow the patient to swallow them, they should be crushed one at a time and not mixed. This will allow the administrator to tell drugs apart if there is a spill or if the patient refuses some of them. Mixing crushed medications in a small amount of soft food, such as applesauce or pudding may facilitate easier swallowing.
Position the patient in a side-lying or upright position to decrease the risk of aspiration. Offer a glass of water or other oral fluid (that is not contraindicated with the medication) to ease swallowing and improve absorption and dissolution of the medication, taking any fluid restrictions into account. Remain with the patient until all medication has been swallowed. Sign for the medication AFTER the medication has been swallowed / administered.
Checklist 45 outlines the steps for administering medication by mouth.
Checklist 45: Administering Medication by MouthDisclaimer: Always review and follow your agency policy regarding this specific skill. |
|||
Safety considerations:
|
|||
Steps |
Additional Information |
||
| 1. Perform hand hygiene before medication preparation.
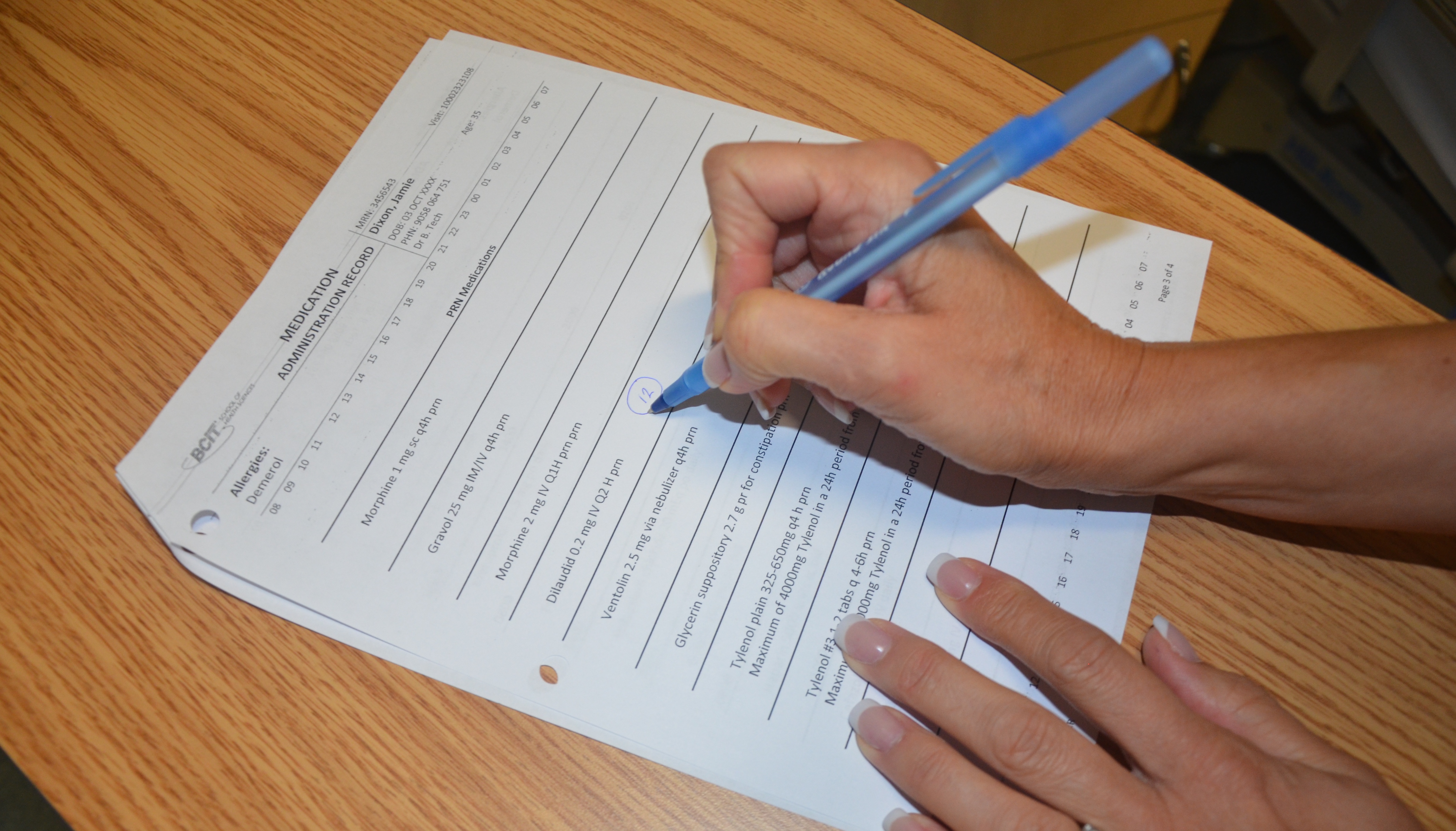
Check MAR to guide you to which medications you are preparing. Follow agency policy to ensure MARs are accurate and verified appropriately. |
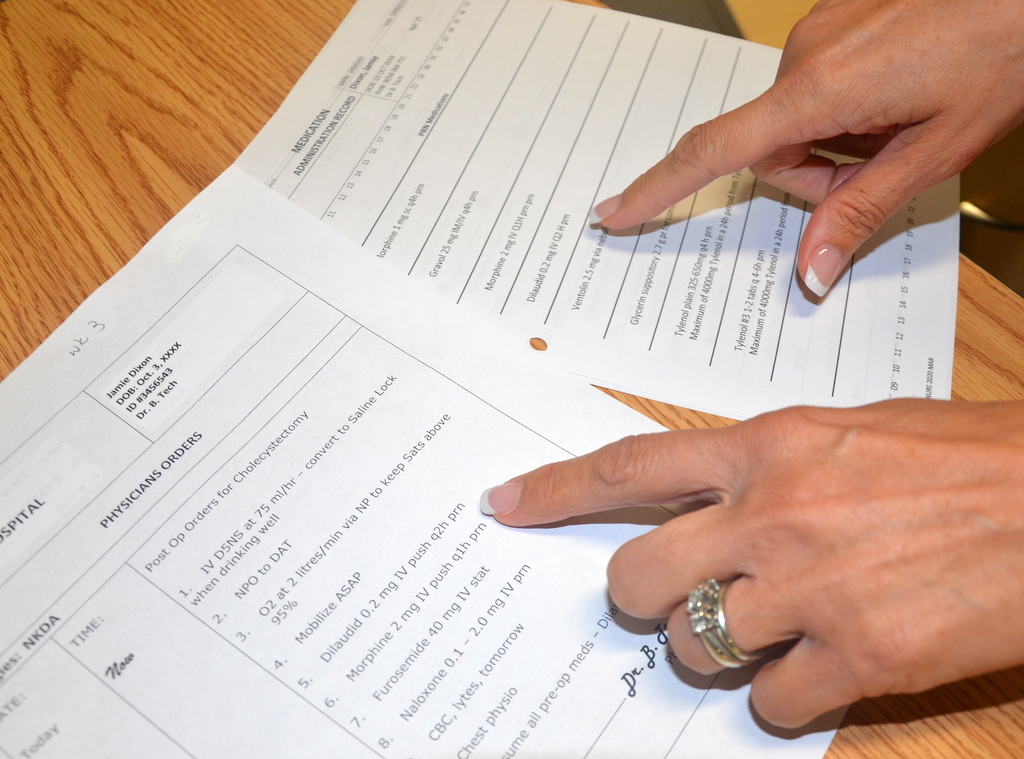 An MAR that is checked by more than one healthcare professional provides a very reliable record for administering medications. Agencies may vary in relation to MAR verification processes. |
||
2 a. As you are removing medications from the dispensing system, perform the SEVEN rights three times with each individual medication: (single dose packaging is not opened at this time)
Perform any necessary medication calculations. Medication calculation: D/H × S = A D (desired dosage) / H (have available) × S (stock) = A (amount prepared) Example order: Liquid sunshine 5 mg PO now. Desired 5 mg/Have 1 mg × Stock 4 ml = A 20 ml  |
The right patient: Check that you have the correct patient using two patient identifiers (e.g., name and date of birth). The right medication (drug): Check that you have the correct medication and that it is appropriate for the patient in the current context. The right dose: Check that the dose makes sense for the age, size, and condition of the patient. Different dosages may be indicated for different conditions. The right route: Check that the route is appropriate for the patient’s current condition. The right time: Adhere to the prescribed dose and schedule. Determine if oral meds should be taken on an empty stomach. The right reason: Check that the patient is receiving the medication for the appropriate reason. The right documentation: Always verify any unclear or inaccurate documentation prior to administering medications.
|
||
2 b. The label on the medication must be checked for name, dose, and route, and compared with the MAR at three different times:
|
 Whenever possible, take the MARs to the bedside and open medication packages at the bedside. Some liquid medications require shaking prior to dispensing. If using an oral syringe, ISMP recommends the use of a special oral medication syringe. These are different than the Luer lock syringes used for parenteral medication administration. |
||
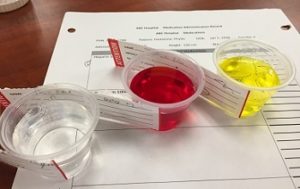
| 2 c. As medications are taken from the drawer / dispensing system, identify on the MAR when a medication is obtained.
Single dose packages are not opened at this time. Liquids or meds from bulk containers can be poured into med cups and labeled. 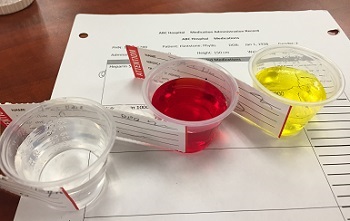 |
 Helps you to keep track of what you’ve obtained and what you haven’t. Meds that are prepared away from the bedside (i.e., liquids, injectables) are labeled before being brought to the bedside.  |
||
3. Take medications and MARs to the bedside:
|
MARs cannot be taken into rooms where additional precautions are required.
 The patient has the right to be informed, and providing reasons for medication, actions, and potential adverse effects may improve adherence to medication therapy and patient reporting of adverse effects. |
||
| 4. Open packages, putting them into an appropriate medication cup. Complete three checks. | Do not touch any medication with ungloved hands. Use clean gloved hands if it is necessary to touch the medication.
Scored tablets can be cut and reliably provide accurate dosing because of evenly dispersed medication in each half of the medication. Chemotherapy drugs are toxic to the administrator. Use gloves when preparing these kinds of medications. If a patient expresses concerns over medications, STOP. Do not give medication. Verify prescriber’s order and explore patient concerns. Notify prescriber if necessary. |
||
5. Positioning
|
 Correct positioning reduces risk of aspiration during swallowing. Water or other oral fluids will help with swallowing of medication. Proper body mechanics reduces risk of injury to health care provider. |
||
6. Administer medication orally as prescribed.
|
Follow any specific descriptions for administration of the medication.
Wear gloves if placing the medication inside the patient’s mouth to protect the healthcare worker from BBF exposure and to reduce risk of absorbing the medication through the skin. |
||
7. Post-medication safety check:
|
Right documentation includes signing for medications after administration.
Document any additional information, such as patient education, reasons why medication not administered, and adverse effects, as per agency policy. Post assessments determine effectiveness and potential adverse effects of medications. |
||
| 8. Return within appropriate time to evaluate patient’s response to the medications and to check for possible adverse effects.
If patient presents with any adverse effects:
|
Most sublingual medications act in 15 minutes, and most oral medications act in 30 to 40 minutes.
|
||
| Data sources: BCIT, 2015; ISMP, 2011; Lilley et al., 2016; Perry et al., 2018 | |||
Administering Medication via a Gastric Tube
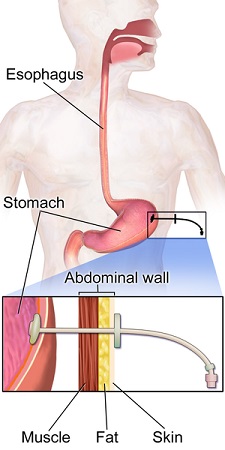
Patients with a gastric tube (nasogastric, nasointestinal, percutaneous endoscopic gastrostomy [PEG], or jejenostomy [J] tube) will often receive medication through this tube (Lynn, 2011). Liquid medications should be used when possible because absorption is better and less likely to cause blockage of the tube. Liquid forms of medication should be used when possible. However, some solid forms of medication can be crushed and mixed with water for administration. Important safety considerations for administering medications via this route include knowing which medications can be crushed and which can’t; verify tube placement; elevate the head of bed to at least 30 degrees to decrease risk of aspiration; flush with water before and after each medication to reduce risk of blockage; dilute medications with water and administer one medication at a time to prevent tube blockage.
If a tube feed is infusing, temporarily stop it for medication administration. If medications need to be given on an empty stomach, stop the tube feed for approximately 30 minutes prior and resume the feed 30 to 40 minutes after. If the patient has one of these tubes for gastric decompression, you will need an order to administer medications via this route. It is also important to keep the tube clamped for 30 to 40 minutes afterward to allow for medication absorption.
Checklist 46 outlines the steps for administering medication via a gastric tube.
Checklist 46: Administering Medication via a Gastric TubeDisclaimer: Always review and follow your agency policy regarding this specific skill. |
|||
Safety considerations:
|
|||
Steps |
Additional Information |
||
| 1. Perform hand hygiene before medication preparation.
Check MAR to guide you to which medications you are preparing. Follow agency policy to ensure MARs are accurate and verified. If a tube feed is infusing, temporarily stop it for medication administration. |
An MAR that is checked by more than one healthcare professional provides a very reliable record for administering medications. Agencies may vary in relation to MAR verification processes. |
||
2 a. As you are removing medications from the dispensing system, perform the SEVEN rights three times with each individual medication: (single dose packaging is not opened at this time)
Perform any necessary medication calculations. Medication calculation formula: Want / Have × Drug form = Amount prepared Order: Liquid sunshine 5 mg PO now. Want 5 mg / Have 1 mg × D 4 ml = 20ml |
The right patient: Check that you have the correct patient using two patient identifiers (e.g., name and date of birth). The right medication (drug): Check that you have the correct medication and that it is appropriate for the patient in the current context. The right dose: Check that the dose makes sense for the age, size, and condition of the patient. Different dosages may be indicated for different conditions. The right route: Check that the route is appropriate for the patient’s current condition. The right time: Adhere to the prescribed dose and schedule. Determine if oral meds should be taken on an empty stomach. The right reason: Check that the patient is receiving the medication for the appropriate reason. The right documentation: Always verify any unclear or inaccurate documentation prior to administering medications.  |
||
2 b. The label on the medication must be checked for name, dose, and route, and compared with the MAR at three different times:
|
Whenever possible, take the MARs to the bedside and open medication packages at the bedside. |
||
| 2 c. As medications are taken from the drawer / dispensing system, identify on the MAR when a medication is obtained.
Single dose packages are not opened at this time.  Liquids or meds from bulk containers can be poured into med cups and labeled. |
Helps you to keep track of what you’ve obtained and what you haven’t. Meds that are prepared away from the bedside (i.e., liquids, injectables) are labeled before being brought to the bedside to help ensure right drug. |
||
| 3. If necessary, crush any tablets. | EC (enteric coated), LA (long acting), SR (sustained release) medications cannot be crushed. Some capsules cannot be opened. Consult the pharmacy and agency guidelines for clarification. | ||
4. Take medications and MARs to the bedside.
|
MARs cannot be taken into rooms where additional precautions are necessary.
The patient has the right to be informed. Providing reasons for medication, actions, and potential adverse effects may improve adherence to medication therapy and patient reporting of adverse effects. Determine if medication should be given with or without food. If the medication is to be given on an empty stomach, the enteral feeding may need to be stopped from 30 minutes before and until approximately 60 minutes after the medication is given. |
||
| 5. Open medications each into its own medication cup. Complete three checks.
Dilute each medication with approximately 20 ml warm water to each medication cup. |
Warm water helps to dissolve the medication allowing it to be administered. Dilution reduces risk of tube blockage.
 |
||
| 6. Anyone with an NG should be positioned with the head of bed at 30-45 degrees. | This position reduces risk of aspiration. | ||
| 7. Apply clean non-sterile gloves. | Using gloves protects the healthcare worker from BBF exposure. | ||
| 8. Check gastric tube for correct placement as described in Chapter 10. | Always trace tubes back to their point of origin and confirm the kind of tube.
|
||
| 9. Remove plunger from a 60 ml catheter tip syringe, and attach syringe to the end of the gastric tube while pinching the gastric tube. | Make sure the tip of the syringe fits the end of the gastric tube.
Pinching the tube prevents reflux of tube feed / gastric secretions onto the patient and bedding. |
||
| 10. Flush with 30 ml of warm water before medication.
Pour prepared medication into the 60 ml syringe, release pinch, and allow fluid to drain slowly by gravity into the gastric tube Flush tube with 15 ml of water between each medication. Flush with 30 ml warm water after medication. |
Flush using a 60 ml syringe with appropriate tip to access the G tube. Use a push / pause technique to clean the lumen of the tube.
Administering one medication at a time reduces risk of medication interactions and blockage of the tube. Water flushes before, between, and after medications cleanses the tube’s lumen and reduces risk of medication interaction and risk of tube blockage. If fluid does not drain by gravity, gentle pressure may be applied using the plunger of the syringe, but do not force the medication through the tube. 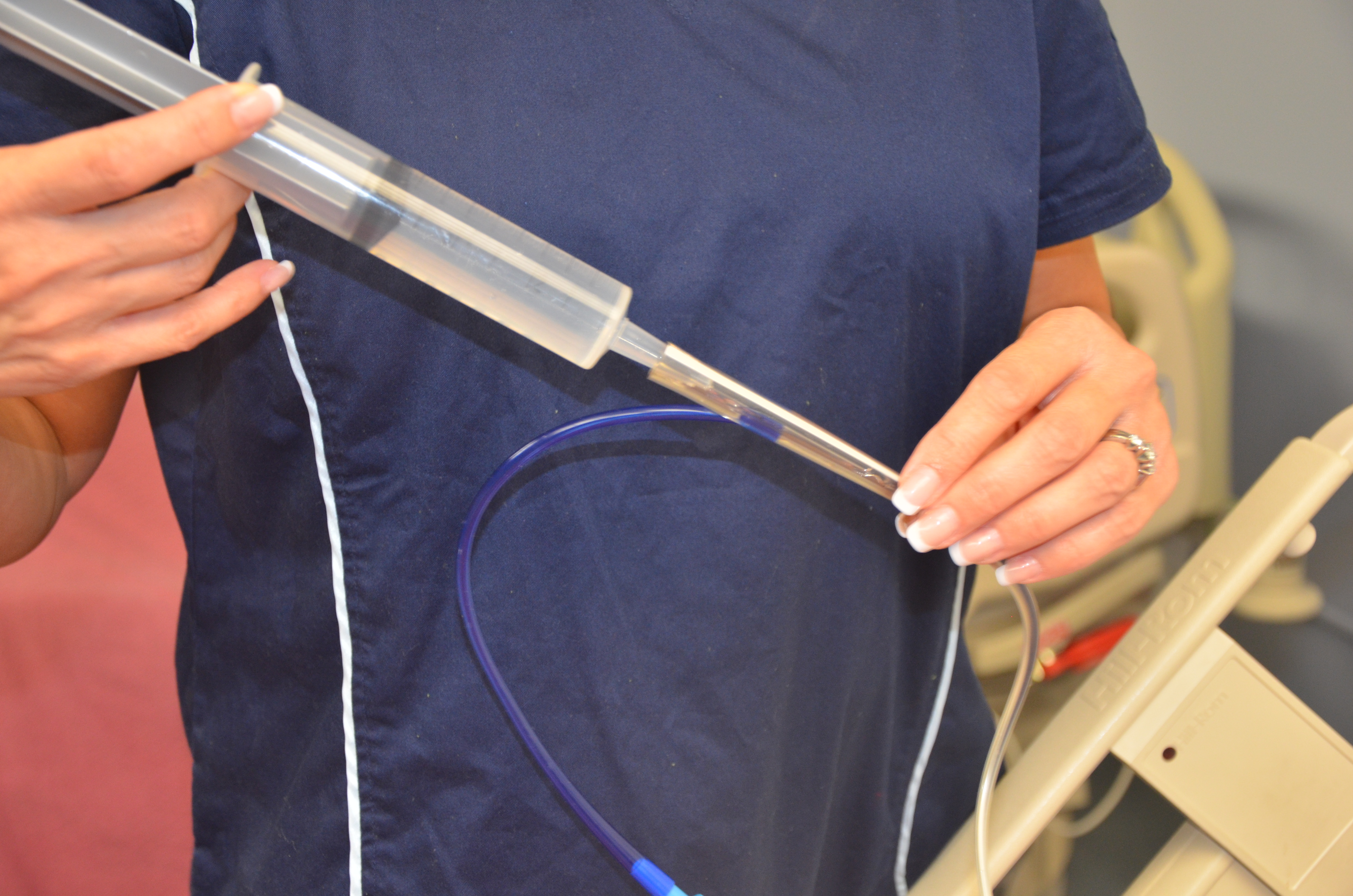 |
||
11. Post-medication safety check:
|
If this is a tube intended for gastric decompression, clamp for 30 to 60 minutes then resume gastric suction. If this tube is used for enteral feeds, resume feed.
|
||
| 12. Return within appropriate time frame to evaluate patient’s response to the medications and to check for possible adverse effects.
If patient presents with any adverse effects:
|
Evaluate patient for intended and adverse effects. | ||
| Data sources: BCIT, 2015; Boulatta, 2009; Lilley et al., 2016; Perry et al., 2018; RCH, 2017; Saskatoon Health Region, 2017 | |||

Critical Thinking Exercises
- Your patient is dysphagic. Discuss the steps you should take and the considerations you should be cognizant of to administer oral medication safely.
- Your patient is unable to swallow and is receiving medication and nutritional sustenance via an enteral jujenostomy tube. The drug reference guide recommends that medication should be given on an empty stomach. Discuss how you would approach this situation.
Attributions
Figure 6.2. Bunch of pills by E-magine Art is used under a CC BY 2.0 license.
Figure 6.3. Liquid sunshine by author is licensed under a Creative Commons Attribution 4.0 International License.
Figure 6.4. Three liquid meds with labels by author is licensed under a Creative Commons Attribution 4.0 International License.
Figure 6.5 Meds and MARs at bedside by author is licensed under a Creative Commons Attribution 4.0 International License.
Figure 6.6. Illustration depicting a gastric feeding tube for an adult by BruceBlaus is used under a CC BY-SA 4.0 International license.
Figure 6.7. Liquid med with label by author is licensed under a Creative Commons Attribution 4.0 International License.

{kind=link}