Chapter 7. Parenteral Medication Administration
7.6 Intravenous Medications by Direct IV (Formerly IV Push)
In the past, IV medications given as described above were referred to as IV bolus or IV push medications. It is recommended that these terms NOT be used, as they can be mistakenly interpreted as meaning the drugs are to be pushed quickly, in less than a minute (ISMP, 2003). To administer IV medications safely and effectively, nurses must follow all agency policies and use PDTM guidelines to determine which medications can be given intravenously and any specific instructions about administration (Alberta Health Services, 2009).
Intravenous (IV) is a route for administering concentrated medications (diluted or undiluted) directly into the vein. Depending on the medication and the purpose, meds given IV may be through continuous infusions, mini-bags, or more quickly by what is referred to as direct IV. The IV direct route refers to the administration of a small volume of fluid / medication (max. 20 ml) pushed manually into the patient using a syringe Leur locked to a needleless port. Medications given by direct IV are usually administered intermittently to treat emergent concerns. Medications administered by direct IV route are given very slowly over at least one minute (Perry et al., 2014). The nurse must consult drug monographs and / or Parenteral Drug Therapy Manual (PDTM) for specifics about each medication. Administering a medication intravenously eliminates the process of drug first pass by depositing the medication directly into the blood. This results in the immediate elevation of serum drug levels and high drug concentrations in vital organs, such as the heart, brain and kidneys. Both therapeutic and adverse effects can occur quickly with IV direct administration (Alberta Health Services, 2009).
There are many advantages and disadvantages to administering medications via the intravenous injection method—see Table 7.7.
Intravenous medications are always prepared using the SEVEN rights and THREE checks as per agency policy. Because of the high risk associated with direct intravenous medications, additional guidelines are required. A PDTM or drug monograph provides additional information to help the nurse make decisions about administering IV medications. Some medications can be given either IV direct or piggyback, in which case the nurse must use their knowledge about the patient to determine which of these is preferred. Some medications may only be given in large-volume IV solutions; some medications have to be diluted; some medications have to be administered over specific time frames (i.e., over 1 or 2 minutes). In addition, information regarding indications, contraindications, dosage (age dependent), administration/dilution guidelines, adverse effects, clinical indications (e.g., specialized monitoring required, must be on an IV pump), compatibility and incompatibility in relation to reconstitution and primary IV solution is specified (Alberta Health Services, 2009).
The Institute for Safe Medication Practices (ISMP) (2014) has created a list of high-alert medications that bear the heightened risk of significant harm when they are used in error. Special safeguards for these medications can be found in the PDTM. It is vital to understand which medications are considered high risk prior to administration. A link to the list of high-risk medications can be found under Suggested Online Resources at the end of this chapter. Review the steps shown in Table 7.8 to prepare a medication by direct IV route. The PDTM must be consulted every time an IV medication is given, as memory-based errors are common (World Health Organization, 2012).
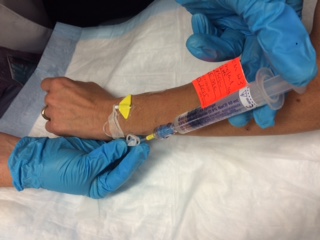
Before giving an intravenous medication, always assess the IV insertion site for patency and for signs of infiltration or phlebitis. Start a new IV site if current site is red, swollen, or painful when flushing. Intravenous medications by direct IV route can be given three ways:
- Through an IV that is capped / locked.
- Through an IV that has an infusion running and the medication is compatible with the IV solution.
- Through an IV that has an infusion running and the medication is incompatible with the IV solution.
Checklist 60 reviews the steps to administer a medication IV direct into a locked / capped IV. Review the preparation questions for intravenous medication in Table 7.8 prior to administering medication.
Checklist 60: Administering Medications IV Direct into a Locked / Capped IV (PVAD Short, Midline, PICC, Percutaneous Non-Hemodialysis CVC)Disclaimer: Always review and follow your agency policy regarding this specific skill. |
|||
Safety considerations:
|
|||
Steps |
Additional Information |
||
| 1. Prepare one medication for one patient at the correct time as per agency policy. Review the physician’s order, PDTM, and MAR for the correct order and guidelines. Math calculations may be required to determine the correct dose to prepare the medication. | Always apply the SEVEN rights and THREE checks of medication administration.
Review the agency policy if a medication is a stat, given for the first time, a loading dose, or a one-time dose. Some agencies require that high-alert medications be double-checked by a second health care provider. Always follow agency policies. For a list of high-alert medications, see Suggested Online Resources. After preparing the medication, always label the medication syringe with two patient identifiers (name & date of birth), date, time, medication, dose (ie. 2 mg), and your initials. Never leave the medication syringe unattended. |
||
| 2. Create privacy if possible. | This provides comfort to patient. | ||
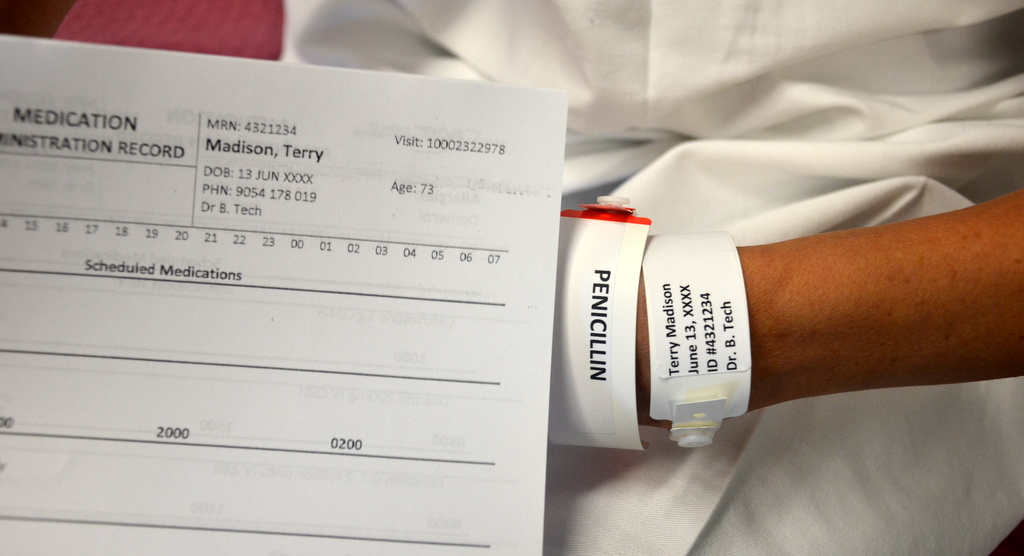
| 3. Confirm patient ID using two patient identifiers (e.g., name and date of birth) AND compare the MAR with the patient’s wristband to confirm patient ID. | This ensures you have the correct patient and complies with agency standard for patient identification.
 |
||
| 4. Check allergy band for any allergies, and ask patient about type and severity of reaction. | This ensures allergy status is correct on the MAR and on patient’s allergy band. | ||
| 5. Discuss purpose, action, and possible side effects of the medication. Provide patient an opportunity to ask questions. Encourage patient to report discomfort at the IV site (pain, swelling, or burning). | Keeping the patient informed of what is being administered helps decrease anxiety. | ||
| 6. Perform hand hygiene | Hand hygiene prevents the transmission of microorganisms. | ||
| 7. Assess IV insertion site for complications. See Checklist 65.
Clean access port / needleless cap using alcohol and friction for 15 seconds. Allow to dry. |
Alcohol and friction sanitizes. Allowing alcohol to dry renders the antiseptic properties effective. Cleaning access ports before each syringe is attached and after each syringe is detached reduces risk of infection.
 |
||
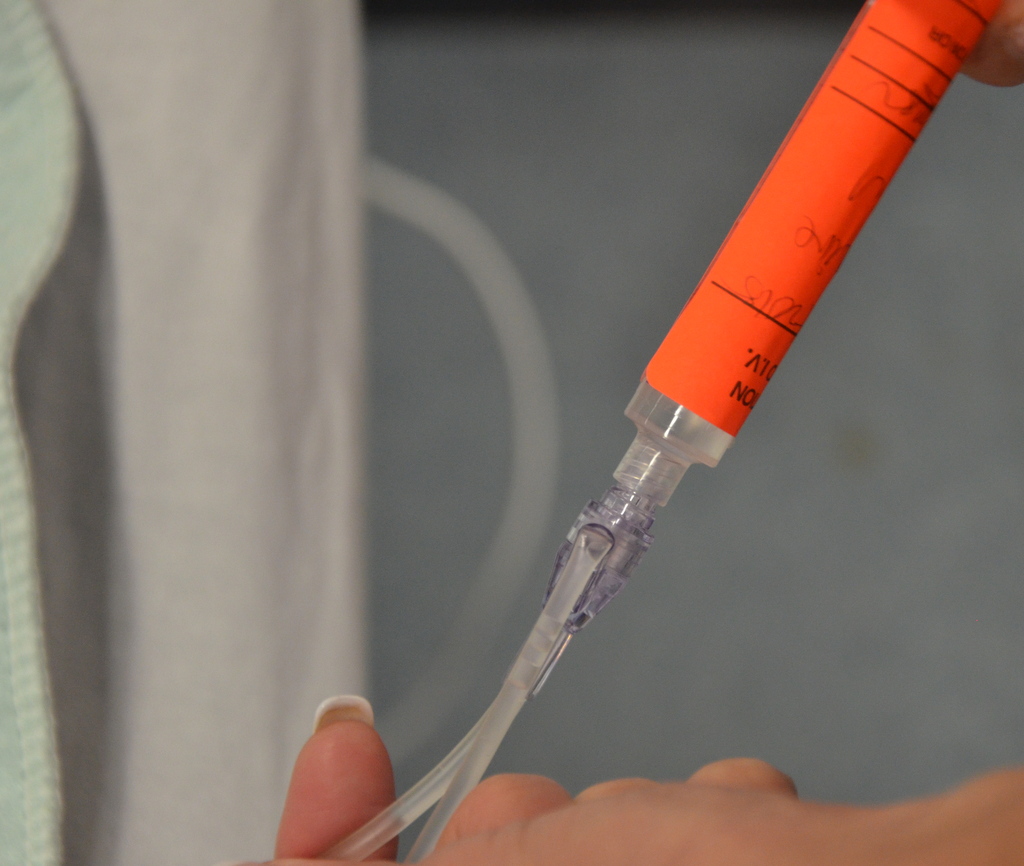
| 8. Luer lock 10 ml saline filled syringe onto needleless cap. Release clamp on extension tubing if present. | 10 ml syringes for flushing reduces risk of fracturing the IV cannula.
 
Refer to agency guidelines for VAD flushing & locking protocols. |
||
| 9. Verify patency of the line.
PVAD short:
Midline, CVC (PICC / percutaneous non-hemodialysis line):
Remove syringe. |
PVAD short: if swelling, pain, or redness exists, remove IV cannula and reestablish new IV site. Tenderness is the first sign of phlebitis.
Aspirating on a PVAD short often does not reveal blood flashback despite the site being patent. Assess for patency of PVAD short during the flush by assessing for resistance, pain, and leaking. If you suspect the line is not patent, STOP. DO NOT forward flush. Remove the PVAD short and reestablish a new one. Turbulent flush is a stop start vigorous motion intended to clean the inside lumen of the VAD.
Aspirating on a PICC, midline, and percutaneous non-hemodialysis CVC should reveal blood flashback. If you suspect the line is not patent, or partially occluded, follow agency guidelines (this usually involves trouble shooting and / or consulting the IV team / PICC nurse for declotting). If possible, aspirate only until flashback of blood is into the catheter. Flashback into syringe creates more risk for occlusion if not flushed correctly. |
||
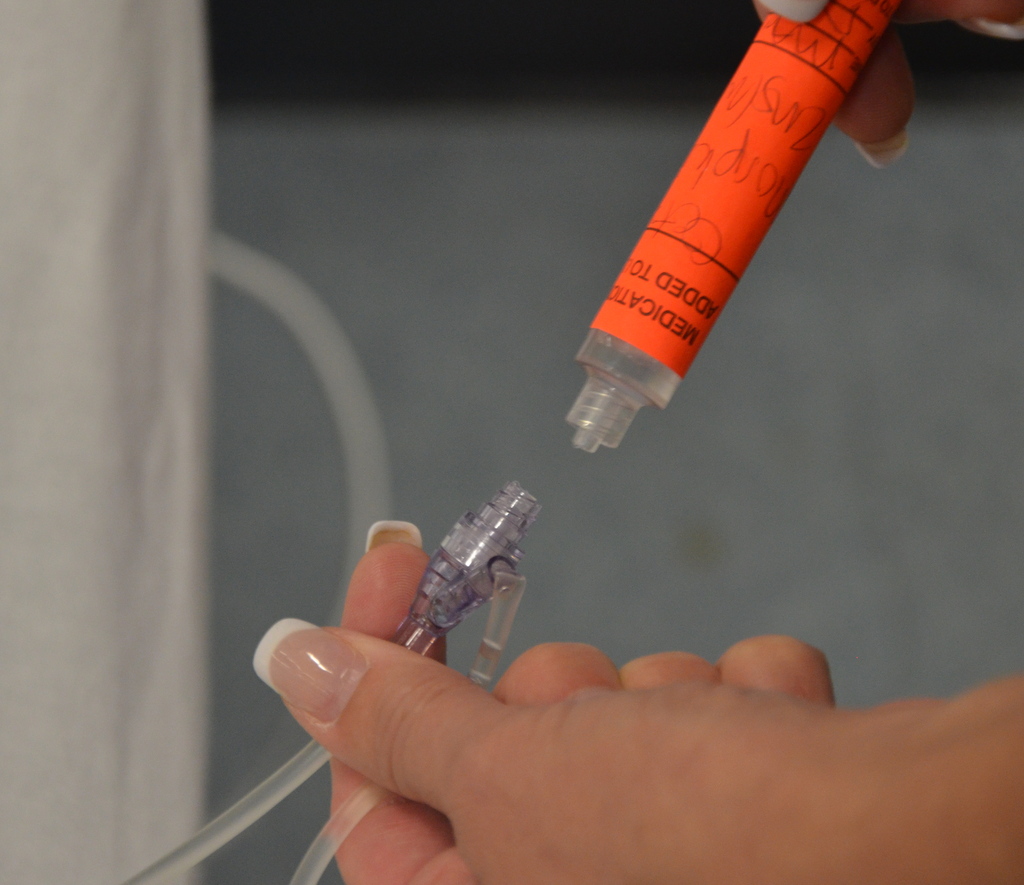
| 10. Clean access port with alcohol and friction for 15 seconds.
Luer lock medication syringe to needleless cap. |
Cleaning access ports before each syringe is attached and after each syringe is detached reduces risk of infection.
Using a needleless system prevents needle-stick injuries. Use 10 ml syringe (minimum) to reduce risk of catheter fracture.  |
||
| 11. Use a timer / watch / clock to inject medication at the correct rate according to agency policy. Administer the medication slowly and steadily. Attempt to have half of the syringe emptied in half of the recommended infusion time. | Timing of the administration promotes safer medication administration. Rapid injection of IV medications can have serious consequences for the patient.
 |
||
| 12. Remove empty medication syringe.
Clean access port using alcohol and friction for 15 seconds.
Luer lock 10 ml saline filled syringe to the needleless cap. Flush with volume directed by agency ‘s flushing protocol at the SAME rate as the medication delivery, according to guidelines found in the PDTM. (See Rationale for Flushing with NS after Administering an IV Medication)
Ensure the final flush is done in a way that ensures positive pressure is achieved. This will depend on what kind of needleless cap and what kind of saline filled syringe is available to you. See Positive Pressure.
|
Cleaning access ports before each syringe is attached and after each syringe is detached reduces risk of infection.
Check agency flushing protocol for flushing volume. Flushing the IV line at the same rate as medication delivery ensures that any medication remaining within the IV line is delivered at the correct rate, and avoids the patient receiving an accidental bolus of the medication.  Flushing the extension tubing clears the medication from the device.  Note: If a patient has a central venous catheter, follow agency protocols for accessing and flushing and locking.
Always assess IV sites before and after administration of IV medications. |
||
| 13. Dispose of all syringes, blunt fill needles, blunt fill filter needles according to agency policy. | This prevents accidental needle-stick injuries. | ||
| 14. Perform hand hygiene. | This reduces transmission of microorganisms. | ||
| 15. Document as per agency protocol. | Document the time, reason, drug, dose, effect, and any adverse reactions. | ||
| 16. Observe for expected therapeutic effect and for adverse effects. | The patient needs to be evaluated and monitored, especially for high-alert medications. IV medications act rapidly. | ||
| Data source: Canadian Institute for Health Information, 2009; Clayton et al., 2010; Goossens, 2015; Perry et al., 2018 | |||
Special considerations when giving meds IV:
- Top contributing factors to medication errors include calculation errors, drug preparation errors, human error, and transcription inaccuracy.
- The elderly and the young may be more sensitive to adverse effects.
- With certain medications, creatinine clearance must be assessed prior to administering. Patients with liver disease may require a reduction in dosages.
- When a medication dose is ordered with a range (e.g., morphine 2 mg IV q 2-4 hours p.r.n.), always start with the lowest dose and titrate up. Always assess when the last dose was given and its effectiveness.
Considerations for Saline Flushes after IV Medication Administration
- The normal saline flush after IV meds are administered serves a few purposes: 1) to deliver any medication left in the tubing in to the patient; 2) to reduce risk of residue – medications / IV solutions / fibrin- build up in the lumen of the IV cannula (Gossens, 2015); and 3) to establish an environment within the IV cannula to prevent reflux of blood and / or clotting of the VAD if it is to remain locked
- When meds are given IV direct, some medication remains in the tubing between the access port and the end of the IV cannula. As such care must be taken to complete the flush in a way that does not result in a bolus of medication being administered too quickly. Sudden boluses of some medications may cause mild to severe adverse effects, such as hypotension and toxicity (Clayton et al., 2010).
- The flushing solution must be compatible with other IV solutions / meds
- Turbulent flush is a stop start motion intended to cleanse the inside lumen of the IV cannula.
- High PSI (pounds per square inch) can fracture an IV cannula. Always use the manufacturers guidelines for choosing the syringe size (usually 10 ml).
- Refer to flushing protocols. Open ended CVADs require heparin after the saline flush to reduce risk of clotting.
Here are some examples of clearing IV medication from the extension tubing on a PVAD short saline lock.
- If morphine (1 mg) is administered over one minute, the subsequent saline flush will be given in this manner: the first 1 ml of a 5 ml saline flush will be delivered over one minute to clear the medication from the tubing, and the remaining 4 ml will be the turbulent flush.
- If furosemide (40 mg) is given in a 4 ml volume and administered over two minutes, the subsequent saline flush will be given in this manner: the first 1 ml of a 5 ml saline flush will be delivered over 30 seconds, and the remaining 4 ml will be the turbulent flush.
Checklist 61 lists the steps to administering an IV medication through an existing IV line with compatible IV solution. Review the preparation questions for intravenous medication in Table 7.8 prior to the medication administration.
Checklist 61: Administering medications IV direct into an infusing IV – with compatible solution (PVAD short, midline, PICC, percutaneous non-hemodialysis CVC)Disclaimer: Always review and follow your agency policy regarding this specific skill. |
|||
Safety considerations:
|
|||
Steps |
Additional Information |
||
| 1. Prepare one medication for one patient at the correct time as per agency policy. Review the physician’s order, PDTM, and MAR for the correct order and guidelines. Math calculations may be required to determine the correct dose to prepare the medication.
Determine compatibilities of the medication to be given with the primary IV solution. If the primary solution contains medication that should not be stopped (e.g., heparin, morphine, pantoprazole, insulin, or blood or blood products), do not use this line. In this case establish another IV access. |
Always apply the SEVEN rights and THREE checks of medication administration.
Review the agency policy if a medication is a stat, first-time, loading dose, or a one-time dose. Some agencies require high-alert medications to be double-checked by a second health care provider. Always follow agency policies. After preparing the medication, always label the medication syringe with two patient identifiers, date, time, medication, dose (e.g., morphine 2 mg), and your initials. Never leave the syringe unattended. If medications given simultaneously are incompatible, the mixing of these can create precipitates in the IV tubing which can initiate emboli formation in the blood. Stopping infusions that containing medications interrupts delivery of that medication. Blood and blood products are NOT compatible with ANY medication. |
||
| 2. Create privacy if possible. | This provides comfort to patient. | ||
| 3. Confirm patient ID using two patient identifiers (e.g., name and date of birth) AND compare the MAR printout with the patient’s wristband to confirm patient ID. | This ensures you have the correct patient and complies with agency standard for patient identification.
 |
||
| 4. Check allergy band for any allergies, and ask patient about type and severity of reaction. | This ensures allergy status is correct on the MAR and on patient allergy band. | ||
| 5. Discuss purpose, action, and possible side effects of the medication. Provide patient an opportunity to ask questions. Encourage patient to report discomfort at the IV site (pain, swelling, or burning). | Keeping patient informed of what is being administered helps decrease anxiety. | ||
| 6. Perform hand hygiene | Prevents the transmission of microorganisms. | ||
| 7. Assess IV insertion site. See Checklist 65. | Redness, swelling and leaking suggest complications. | ||
8. Select IV access port closest to the patient. Clean access port using friction with an alcohol swab for 15 seconds. Allow to dry.
 |
The closest port allows the medication to reach the blood stream quickly.
Cleaning access ports before each syringe is attached and after each syringe is detached reduces risk of infection. Alcohol and friction sanitizes. Allowing alcohol to dry renders the antiseptic properties effective. Refer to agency guidelines for VAD flushing & locking protocols. |
||
| 9. Stop the infusion. | Stopping the infusion for an IV run by gravity involves clamping a slide clamp distal to the access port or rolling the roller clamp to the closed position OR folding the tubing on itself and pinching it.
Stopping the infusion for an IV run by an EID / pump simply involves stopping the machine. |
||
| 10. Verify site patency.
Luer lock a 10 ml saline filled syringe to the access port closest to the patient. Aspirate and assess for blood flashback in the line. Forward flush 10 ml normal saline syringe using turbulent technique. THIS IS THE FLUSH PRIOR.
|
Checking patency of PVAD short: you can aspirate… or not. Likely you can assess patency through observation of the site with an infusing IV. PVAD short sites that are not patent may be edematous (suggests infiltration), may not be infusing (observe for drops in the drip chamber) or the EIDs / IV pumps alerts presence of an occlusion.
Checking patency of midline, CVC (PICC / non-hemodialysis line): aspirate for blood return. When blood flashback present in tubing, forward flush using turbulent technique. If there is no blood return, trouble shoot according to agency protocol and / or contact the IV team / PICC nurse for further assessment. Using a needleless system prevents needle-stick injuries. New recommendations include flushing before AND after medication administration. 10 ml syringes decrease risk of catheter fracture. Flushing the line clears aspirated blood and reduces risk of clotting and occlusion. Turbulent flush cleans IV lumen of medication residue and fibrin. DO NOT force if resistance is felt. |
||
| 11. Remove syringe.
Clean IV access port for 15 seconds with alcohol and friction. Allow to dry.
Luer lock medication syringe to the access port. |
Cleaning access ports before each syringe is attached and after each syringe is detached reduces risk of infection.
|
||
| 12. Inject medication at the recommended rate according to PDTM. Use a timer / watch / clock to monitor time. Administer the medication slow and steady. Attempt to have half of the syringe emptied in half of the recommended infusion time. | Timing of the administration promotes safer medication delivery. Rapid injection of IV medications can have serious consequences for the patient | ||
| 13. Remove empty medication syringe.
Clean port using alcohol and friction.
Luer lock a 10 ml saline filled syringe to the access port.
Flush with volume directed by agency flushing protocol at the SAME rate as the medication delivery, according to guidelines found in the PDTM. (See Rationale for Flushing with NS after Administering an IV Medication.) THIS IS THE FLUSH AFTER.
Resume the infusion.
|
 Alcohol and friction sanitizes. Allowing alcohol to dry renders the antiseptic properties effective. Cleaning access ports before each syringe is attached and after each syringe is detached reduces risk of infection. The final flush does NOT have to ensure positive pressure is achieved because the infusion will be resumed. Always assess IV sites before and after administration of IV medications. |
||
| 14. Dispose of all syringes, and blunt fills and blunt fill filters as per agency protocol. | Blunt fill and blunt fill filters are disposed of in sharps containers to prevent accidental needle-stick injury. | ||
| 15. Perform hand hygiene. | This reduces transmission of microorganisms. | ||
| 16. Document as per agency protocol. | Document time, reason, drug, dose, therapeutic effect, and any adverse reactions. | ||
| 17. Evaluate the patient for therapeutic effect and adverse reactions according to appropriate time frame (onset and peak of medication). | Observations provide additional safety measures, especially for high-alert medications. IV medications act rapidly. | ||
| Data source: Berman & Snyder, 2016; Canadian Institute for Health Information, 2009; Clayton et al., 2010; Perry et al., 2018; Workers Compensation Act, 2015 | |||
Checklist 62 reviews the steps to administer an IV medication through an existing IV line with incompatible IV solution. Review the preparation questions for intravenous medication in Table 7.8 prior to the medication administration.
Checklist 62: Administering Medications IV Direct into an Infusing IV with Incompatible IV Solution (PVAD Short, Midline, PICC, Percutaneous Non-Hemodialysis CVC)Disclaimer: Always review and follow your agency policy regarding this specific skill. |
|||
Safety considerations:
|
|||
Steps |
Additional Information |
||
| 1. Prepare one medication for one patient at the correct time as per agency policy. Review the physician orders, PDTM, and MAR for the correct order and guidelines. Math calculations may be required to determine the correct dose to prepare the medication.
Always check agency policy to ensure an IV solution or medication can be stopped temporarily (i.e., longer than it takes to check patency). Some IV solutions (i.e., those with medications in the primary solution—insulin, heparin) can not be stopped. If unable to temporarily stop an IV solution or IV medication, establish a new IV access at a different site. |
Always apply the SEVEN rights THREE checks of medication administration.
Review the agency policy if a medication is a stat, first-time, loading dose, or a one-time dose. Some agencies require that high-alert medications be double-checked by a second health care provider. Always follow agency policies. After preparing the medication, always label the medication syringe with two patient identifiers, date, time, medication and dose (e.g., morphine 2 mg), dose, and your initials. Never leave the syringe unattended.
|
||
| 2. Create privacy if possible. | This provides comfort to patient. | ||
| 3. Confirm patient ID using two patient identifiers (e.g., name and date of birth) AND compare the MAR printout with the patient’s wristband to confirm patient ID. | This ensures you have the correct patient and complies with agency standard for patient identification.
|
||
| 4. Check allergy band for any allergies, and ask patient about type and severity of reaction. | This ensures allergy status is correct on the MAR and on patient allergy band. | ||
| 5. Discuss purpose, action, and possible side effects of the medication. Provide patient an opportunity to ask questions. Encourage patient to report discomfort at the IV site (pain, swelling, or burning). | Keeping patient informed of what is being administered helps decrease anxiety. | ||
| 6. Perform hand hygiene | Hand hygiene prevents the transmission of microorganisms. | ||
| 7. Assess IV insertion site. See Checklist 65 | Redness, swelling and leaking suggest complications. | ||
| 8. Select IV access port closest to the patient. Clean access port using friction with an alcohol swab for 15 seconds. Allow to dry.
|
The closest port allows the medication to reach the blood stream quickly.
Cleaning access ports before each syringe is attached and after each syringe is detached reduces risk of infection. Alcohol and friction sanitizes. Allowing alcohol to dry renders the antiseptic properties effective.
Refer to agency guidelines for VAD flushing & locking protocols. |
||
| 9. Stop the infusion.
|
Stopping the infusion for an IV run by gravity involves clamping a slide clamp distal to the access port or rolling the roller clamp to the closed position OR fold the tubing on itself and pinch
Stopping the infusion for an IV run by an EID / pump simply involves stopping the machine. |
||
| 10. Verify site patency
Luer lock a 10 ml saline filled syringe to the access port closest to the patient. Aspirate and assess for blood flashback in the line. Forward flush 10 ml syringe using turbulent technique.
THIS FLUSH WILL CLEAR THE LINE OF THE INCOMPATIBLE MEDICATION.
|
Checking patency of PVAD short: you can aspirate… or not. Likely you can assess patency through observation of the site with an infusing IV.
PVAD short sites that are not patent may be edematous (suggests infiltration) or not infusing (observe for drops in the drip chamber); or the IV pump indicates occlusion.
Checking patency of midline, CVC (PICC / non-hemodialysis line): aspirate for blood return. When blood flashback is present in tubing, forward flush using turbulent technique. If there is no blood return, trouble shoot according to agency protocol and / or contact the IV team / PICC nurse for further assessment.
Using a needleless system prevents needle-stick injuries. 10 ml syringes decrease risk of catheter fracture. Flushing the line clears aspirated blood and reduces risk of clotting and occlusion and it clears the line of incompatible medication. Turbulent flush cleans IV lumen of medication residue and fibrin. DO NOT force if resistance is felt. |
||
| 11. Remove syringe.
Clean IV access port for 15 seconds with alcohol and friction. Allow to dry. |
Cleaning access ports before each syringe is attached and after each syringe is detached reduces risk of infection.
The IV line must remain clamped (shut off) to avoid accidental mixing of incompatible IV solution and the medication. |
||
| 12. Leur lock the medication syringe to the access port.
Inject medication at the recommended rate according to PDTM. Use a timer / watch / clock to monitor time. Administer the medication slow and steady. Attempt to have half of the syringe emptied in half of the recommended infusion time.
Remove empty syringe. Clean port for 15 seconds using alcohol and friction. Attach a 10 ml normal saline syringe. Flush with volume directed by agency flushing protocol at the SAME rate as the medication delivery, according to guidelines found in the PDTM. (See Rationale for Flushing with NS after Administering an IV Medication.) THIS FLUSH REMOVES MEDICATION FROM THE TUBING.
|
This ensures safe medication administration at the correct rate. Rapid injection of IV medications can have serious consequences for the patient
Always assess IV sites before and after administration of IV medications.
This step delivers the medication that remains in the IV tubing at the same rate, and prevents patient from accidentally receiving a bolus of the medication. It also clears the IV line to prevent any mixing of incompatible medication with the IV solution. The IV line must remain clamped to avoid accidental mixing of incompatible IV solution and the medication. |
||
13. Resume the IV infusion
Assess the IV site.
|
 
Resume the IV infusion |
||
| 14. Dispose of all syringes and blunt fills and blunt fill filters as per agency protocol.
Perform hand hygiene. |
Blunt fill and blunt fill filters are disposed of in sharps containers to prevent accidental needle-stick injury.
This reduces the transmission of microorganisms. |
||
| 15. Evaluate the patient’s response to the medication in the appropriate time frame.
Document according to agency protocol |
Observe patient for expected therapeutic effects and adverse reactions.
Observations provide additional safety measures, especially for high-alert medications. IV medications act rapidly. |
||
| Data source: Berman & Snyder, 2016; Canadian Institute for Health Information, 2009; Clayton et al., 2010; Perry et al., 2014 | |||
Critical Thinking Exercises
- Find a resource that will advise you about onset, peak, and duration of morphine IV.
- What information should be on the label of an IV medication syringe after it is prepared?
Attributions
Figure 7.20 Cleaning access port by author is licensed under a Creative Commons Attribution 4.0 International License.
Figure 7.30 Leur lock syringe to needleless cap by author is licensed under a Creative Commons Attribution 4.0 International License.
Figure 7.31 Apply slide clamp by author is licensed under a Creative Commons Attribution 4.0 International License.
Figure 7.32 Volumetric infusion pump by
Στέλιος Παρισσόπουλος, ΕΠ ΤΕΙ Αθήνας is licensed under a Creative Commons Attribution-Share Alike 3.0 license

{kind=link}