Chapter 8. Intravenous Therapy
8.12 Parenteral Nutrition (PN)
Parenteral nutrition (PN) is a form of nutritional support given intravenously. PN includes proteins, carbohydrates, fats, vitamins, and minerals. It aims to prevent and restore nutritional deficits, allowing bowel rest while supplying adequate caloric intake and essential nutrients, and removing antigenic mucosal stimuli (Perry et al., 2018; Triantafillidis & Papalois, 2014 ). PN may be short-term or long-term nutritional therapy, and it may be administered in hospital or even at home following extensive patient education. The caloric requirements of each patient are individualized according to the degree of stress, organ failure, and percentage of ideal body weight. PN may be administered as peripheral parenteral nutrition (PPN) or via a central line, depending on the components and osmolality. Central veins are the veins of choice because there is less risk of thrombophlebitis and vessel damage (Chowdary & Reddy, 2010). According to Chowdary & Reddy (2010), candidates for PN are:
-
Patients with paralyzed or nonfunctional GI tract, or conditions that require bowel rest, such as small bowel obstruction, ulcerative colitis, or pancreatitis
-
Patients who have had nothing by mouth (NPO) for seven days or longer
- Critically ill patients
-
Babies with an immature gastrointestinal system or congenital malformations
- Patients with chronic or extreme malnutrition, or chronic diarrhea or vomiting with a need for surgery or chemotherapy
- Patients in hyperbolic states, such as burns, sepsis, or trauma
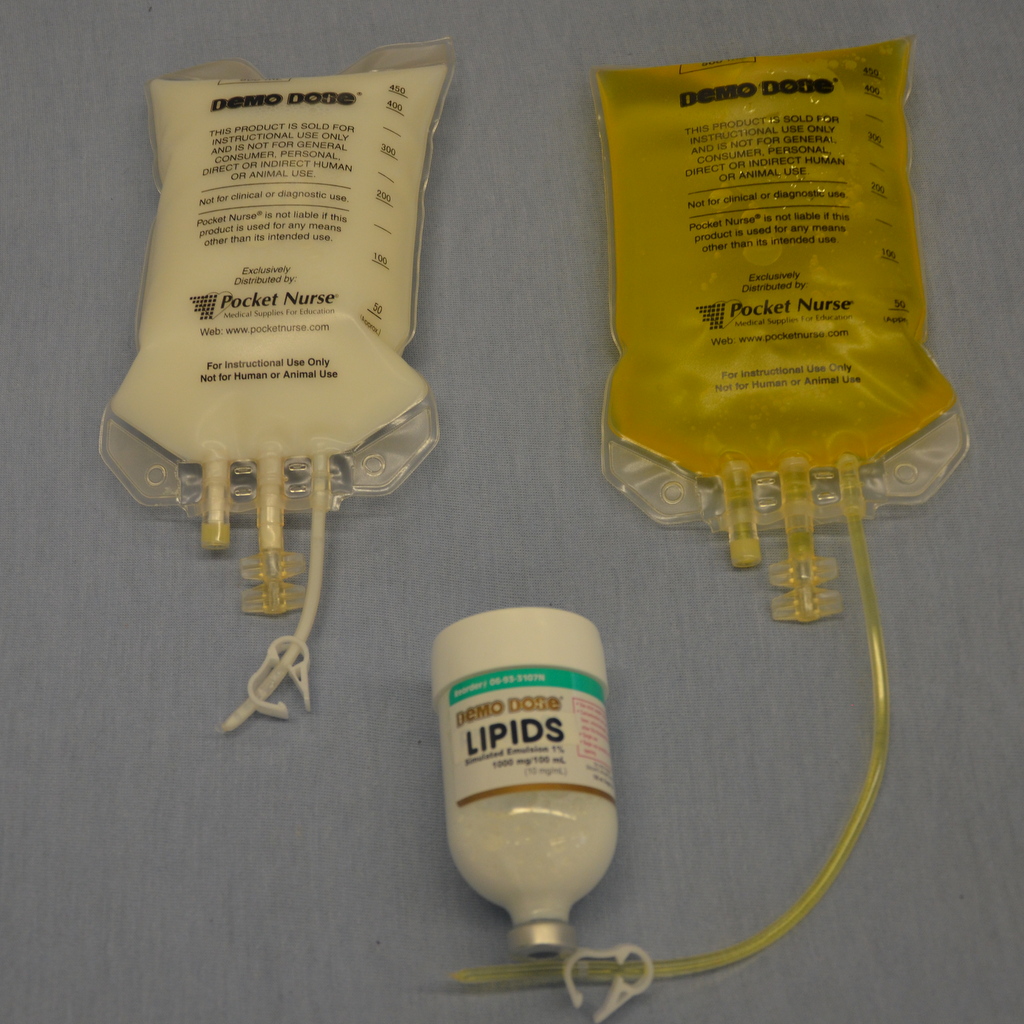
PN is made up of two components: amino acid/dextrose solution and a lipid emulsion solution (see Figure 8.33). The ratios are determined by the dietitian in consultation with the physician and vary depending on the patient’s metabolic needs, clinical history, and blood work. Medications can be added depending on compatibility (for example heparin and insulin are common additives). The solutions are available premixed by the manufacturer. Orders are reviewed daily to ensure the patient receives the solution best suited to their changing needs. The specific mixture, strength, volumes, and any additives must be confirmed by the health care provider every time a new bag is hung.
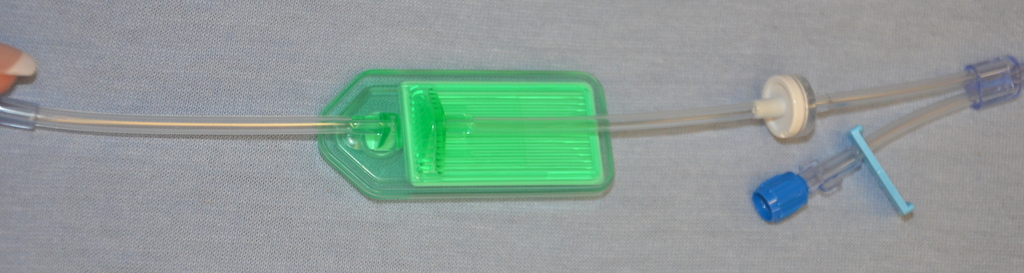
PN is not compatible with other IV solutions, nor is it compatible with many medications. As such, PN should have a dedicated IV line. PN must be administered using an EID (IV pump), and requires special IV filter tubing (see Figure 8.34) for the amino acids and lipid emulsion to reduce the risk of particles entering the patient. Agency policy may allow amino acids and lipid emulsions to be infused together above the filters. PN tubing will not have any access ports and must be changed according to agency policy (usually every 24 hours). Always review agency policy on setup and equipment required to infuse PN.
A prescriber may order a total fluid intake (TFI) for the amount of fluid to be infused per hour to prevent fluid overload in patients receiving PN. It is important to keep track of all the fluids infusing (IV fluids, IV medications, and PN) in order to determine intake and anticipate risk of fluid overload (Perry et al., 2018). Do not abruptly discontinue PN (especially in patients who are on insulin) because this may lead to hypoglycemia. If, for whatever reason, the PN solution runs out while awaiting another bag, hang D5W at the same rate of infusion while waiting for the new PN bag to arrive (North York General Hospital, 2013). Do not obtain blood samples or central venous pressure readings from the same port as PN infusions. To prevent severe electrolyte and other metabolic abnormalities, the infusion rate of PN should be increased gradually, starting at a rate of no more than 50% of the energy requirements (Mehanna, Nankivell, Moledina, & Travis, 2009). Likewise when discontinuing PN, the prescriber might order it to be “weaned” or the rate reduced slowly to prevent hypoglycemia.
Complications Related to PN
There are many complications related to the administration of PN (Perry et al., 2018). Because PN is administered primarily via a CVC, complications associated with CVADs must be considered. See table Table 8.3 Potential Systemic Complications of IV Therapy and Table 8.4 Potential Complications Associated Specifically with CVADs.
Table 8.13 lists PN specific potential complications, rationale, and interventions.
Agencies should have a PN protocol to follow for blood work and other monitoring. Common blood work includes CBC (complete blood count), electrolytes (with special attention to magnesium, potassium, and phosphate), liver enzymes (total and direct bilirubin, alanine aminotransferase [ALT], aspartate aminotransferase [AST], alkaline phosphatase [ALP], gamma-glutamyl transferase [GGT], total protein, albumin), and renal function tests (creatinine and urea). It is important to compare daily values to baseline values, and investigate and report any rapid changes in any values (Chowdary & Reddy, 2010; Perry et al., 2018). Table 8.14 outlines a plan of care for someone receiving PN.
Table 8.14 Plan of Care for Someone Receiving PN |
|||
Assessment |
Additional Information |
||
| CVC/peripheral IV line | Intravenous line should remain patent, free from infection.
Dextrose in PN increases risk of infection. Assess for signs and symptoms of infections at site (redness, tenderness, discharge) and systemically (fever, increased WBC, malaise). Dressing should be dry and intact. |
||
| Daily or biweekly weights | Monitor for evidence of edema or fluid overload. Over time, measurements will reflect weight loss/gain from caloric intake or fluid retention. | ||
| Capillary or serum blood glucose levels | QID (4 times a day) capillary blood glucose initially to monitor glycemic control, then reduce monitoring when blood sugars are stable or as per agency policy. May be done more frequently if glycemic control is difficult. Indicates metabolic tolerance to dextrose in PN solution and patient’s glycemic status. | ||
| Monitor intake and output | Monitor and record every eight hours or as per agency policy. Monitor for signs and symptoms of fluid overload (excessive weight gain) by completing a cardiovascular and respiratory assessment. Assess intakes such as IV (intravenous fluids), PO (oral intake), NG (nasogastric tube feeds). Assess outputs: NG (removed gastric content through the nasogastic tube), fistula drainage, BM (liquid bowel movements), colostomy/ileostomy drainage, closed suction drainage devices (Penrose or Jackson-Pratt drainage) and chest tube drainage. | ||
| Daily to weekly blood work | Review lab values for increases and decreases out of normal range. Lab values include CBC, electrolytes, calcium, magnesium, phosphorus, potassium, glucose, albumin, BUN (blood urea nitrogen), creatinine, triglycerides, and transferrin. | ||
| Mouth care | Most patients will be NPO. Proper oral care is required as per agency policy. Some patients may have a diet order. | ||
| Vital signs | Vital signs are more frequently monitored initially in patients with PN. | ||
| Data sources: BCIT, 2015a; Perry et al., 2018 | |||
Generally, patients receiving PN are quite ill and may require a lengthy stay in the hospital. The administration of PN must follow strict adherence to aseptic technique, and includes being alert for complications, as many of the patients will have altered defence mechanisms and complex conditions (Perry et al., 2018). To administer PN, follow the steps in Checklist 78.
Checklist 78: PN AdministrationDisclaimer: Always review and follow your agency policy regarding this specific skill. |
|||
Safety considerations:
|
|||
Steps |
Additional Information |
||
| 1. Perform hand hygiene.
Review prescribers’ orders and compare to content label on PN solution bag(s) and for rate of infusion. Each component of the PN solution must be verified with the physician’s orders. |
Check date and time of last PN tubing change, lab values, and expiry date of PN to prevent medication error.
Assess CVC, WBC, and patient for malaise. Medications may be added to the PN. Ensure the rate of infusion is verified in the doctor’s order each time new PN bag is initiated. |
||
| 2. Collect supplies, prepare PN solution, and prime IV tubing with filter as per agency protocol. PN requires special IV tubing with a filter. | Generally, new PN tubing is required every 24 hours to prevent catheter-related bacteremia. Follow agency policy.
Ensure tubing is primed correctly to prevent air embolism. |
||
| 3. Perform hand hygiene, identify yourself, and identify patient using two patient identifiers. Compare the label on the PN bag to the patient’s wristband. Explain the procedure to the patient. | Hand hygiene prevents the spread of microorganisms.
Proper identification prevents patient errors.  |
||
| 4. Complete all safety checks for CVC as per agency policy. | This adheres to safety policies related to central line care. | ||
| 5. Complete the flushing protocol as per agency policy.
When changing tubing, sanitize connections and change IV tubing as per agency policy.
|
Ensure patency of all CVCs by completing flushing protocols.
Change PN IV tubing as per agency policy. High dextrose solutions increase risk of developing infections.
|
||
| 6. Insert new PN solution and IV tubing into EID. | EID must be used with all PN administration. | ||
| 7. Start PN infusion rate as ordered. | Prevents medication errors. | ||
| 8. Discard old supplies as per agency protocol, and perform hand hygiene. | These steps prevent the spread of microorganisms. | ||
| 9. Monitor for signs and symptoms of complications related to PN. | See Table 8.13 for list of complications related to PN. | ||
| 10. Complete necessary assessments as per agency guidelines and nursing judgement. | This will include flushing protocols, PN specific potential complications, possible complications related to IV meds (Table 7.10), Potential local complications of IV therapy (Table 8.1), Potential systemic complications of IV therapy (Table 8.3), Potential complications associated specifically with CVADs (Table 8.4) and others. | ||
| 11. Document the procedure in the patient chart as per agency policy. | Note time when PN bag is hung, number of bags, and rate of infusion, assessment of CVC site and verification of patency, status of dressing, vital signs and weight, client tolerance to PN, client response to therapy, and understanding of instructions. | ||
| Data sources: North York General Hospital, 2013; Perry et al., 2018 | |||
Critical Thinking Exercises
- Describe refeeding syndrome and state one method to reduce the risk of refeeding syndrome.
- A patient receiving PN for the past 48 hours has developed malaise and hypotension. What potential complication are these signs and symptoms related to?
Attributions
Figure 8.33 Types of PN from BCIT is used under a CC BY-SA 4.0 international license.
Figure 8.34 PN tubing from BCIT is used under a CC BY-SA 4.0 international license.
