Chapter 2. Patient Assessment
2.3 Pain Assessment
“Pain is whatever the experiencing person says it is, existing whenever the experiencing person says it does” (McCaffery, 1968, as cited in Rosdahl & Kowalski, 2007, p. 704).
Pain is a subjective experience, and self-reporting pain is the most reliable indicator of a patient’s experience (RNAO, 2013). Determining pain is an important component of a physical assessment, and pain is sometimes referred to as the “fifth vital sign.”
 |
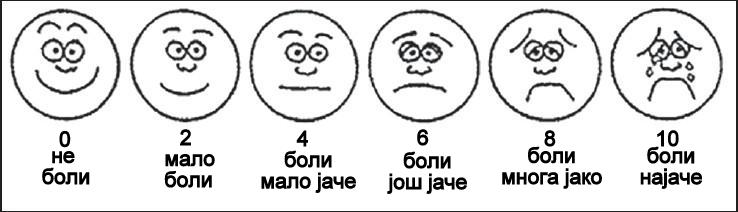 |
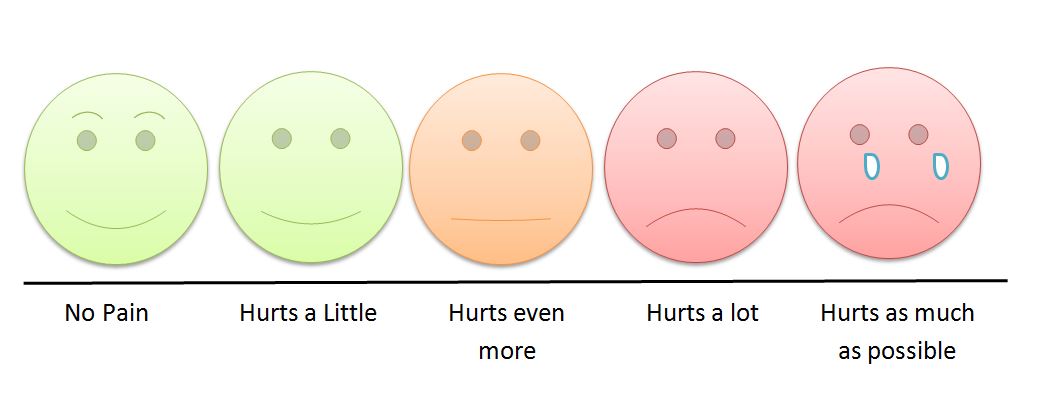
Pain assessment is an ongoing process rather than a single event. A variety of pain assessment tools and visual analogues are available to help with pain assessment (see Figures 2.1 and 2.2). When someone’s pain changes notably from previous findings, a more comprehensive and focused assessment should be performed. Sudden changes may indicate an underlying pathological process (Jarvis, Browne, MacDonald-Jenkins, & Luctkar-Flude, 2014). It is important to assess pain at the beginning of a physical health assessment to determine the patient’s comfort level and potential need for pain comfort measures. Any time you think your patient is in pain, the mnemonic OPQRSTUV may help guide the questions to ask your patient. See Checklist 14 for more specificity regarding this approach.
In their “Clinical Best Practice Guidelines: Assessment and Management of Pain” (2013), the Registered Nurses Association of Ontario (RNAO) has published a variety of pain assessment tools for different populations including children, non-verbal adults, adults with cancer, and neonates. Table 2.1 is an assessment tool that can be used in adults with cognitive impairment.
Table 2.1 Pain Assessment Tools for Elders with Cognitive ImpairmentNote: The screening tool is for the presence/absence of pain but NOT pain intensity. |
|||
Measure |
Characteristics |
Considerations |
|
| Pain Assessment in Advanced Dementia (PAINAD) Scale |
|
|
|
| Pain Assessment Checklist for Seniors with Limited Ability to Communicate (PACSLAC) |
|
|
|
| DOLOPLUS-2 Scale |
|
|
|
| Data source: RNAO, 2013 | |||
Critical Thinking Exercises
- You are caring for a patient who has just returned from a surgical procedure. How might the assessment of acute pain differ from assessment of chronic pain?
- What is more important in pain assessment: the subjective or the objective data?
Attributions
Figure 2.1 Children’s pain scale by Robert Weis is used under a CC BY SA 4.0 licence.
Figure 2.2 The Wong-Baker scale for assessment of pain in children by Intermedichbo is used under a CC BY SA 4.0 licence.

{kind=link}
{kind=link}