Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
Chapter 11: Ostomy care
11.2 Ostomy Care
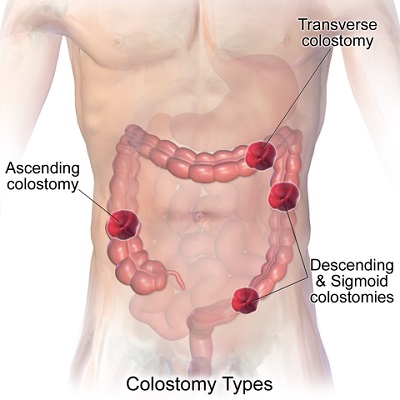
Figure 10.16 Types of ostomies (fecal related)
An ostomy is named according to the part of intestine used to construct it. A colostomy is the creation of a stoma from part of the colon (large bowel), where the intestine is brought through the abdominal wall and attached to the skin, diverting normal intestinal fecal matter through the stoma instead of the anus. An ileostomy is created from the ileum (small bowel), which is brought through the abdominal wall and used to create a stoma. A urostomy or ileal conduit is a stoma created using a piece of the intestine to divert urine to the outside of the body. The ureters are sewn to a piece of the intestine that is made into a small conduit. The conduit emerges from the abdominal wall as a stoma.
These surgeries are performed on patients with diseases such as cancer of the bowel or bladder, inflammatory bowel diseases (such as colitis or Crohn’s), or perforation of the colon. Emergencies that may require an ostomy include diverticulitis, bowel rupture, trauma, necrotic bowel, or radiation complications. An ostomy may be permanent or temporary, depending on the reason for the surgery. Other types of ostomies are called jejunostomy, double-barrel ostomy, and loop ostomy (Perry et al., 2018).
Pouching Systems (Ostomy Appliances)
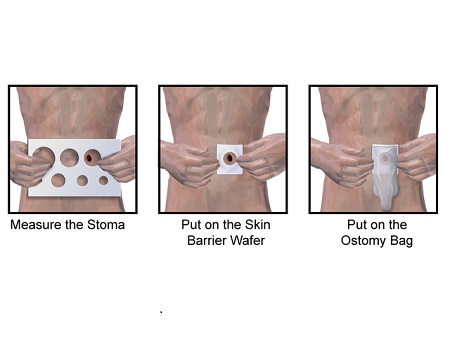
Figure 10.17 Application of ostomy appliance
Individuals with colostomies, ileostomies, or urostomies have no control over the activity of their ostomy. Persons with ostomies must wear a pouching system. The pouching system must be completely sealed to prevent leaking of the effluent and to protect the surrounding peristomal skin. The disposable pouching systems can be either a one-piece or a two-piece system consisting of a pouch (plastic bag) and a flange (skin barrier) that sit against the patient’s skin. Most flanges are flat. Sometimes a stoma that is flat or retracted can be protruded with the use of a convex flange making it easier to direct the drainage into the pouch. The pouch has an open end to allow effluent to be drained, and is closed according to the manufacturer’s design—usually a plastic clip or Velcro strip. Urostomy pouches have a spout type of drainage hole to allow urine to be drained.
Different manufacturers make different types of pouching systems each designed to meet the needs of the client. Step 2 in Checklist 89 shows ostomy supplies including a flange, an ostomy bag, and a one-piece system (Perry et al., 2018; United Ostomy Association of America, 2017). The flange is cut to fit around the stoma in a way that avoids pressure or irritation on the stoma while covering the peristomal skin or a moldable flange can be used to achieve the same result (see Figure 10.18).
Figure 10.18 Moldable flange. Note the turtle-necking of the wafer.
Ostomy pouching systems are chosen based on type of stoma (ileostomy, colostomy, urostomy), stoma characteristics (flat, raised, recessed), stoma location, patient abilities (to cut a flange and to operate the opening / closing of the pouch), skin folds, and patient preference. Pouching systems generally last from four to seven days. Ileosotmies and urostomies generally require more frequent flange changes due to the weight of the effluent and the impact of the weight on the flange’s ability to remain adhered to the patient. The pouch must be changed if it is leaking, if there is excessive skin exposure between the stoma and the edge of the flange (particularly for ileostomies because this stool contains enzymes that break down skin), or if the patient complains of itching or burning under the flange. Patients with established ostomies can swim and participate in most activities of daily life. In terms of showering, pouching systems can remain on or off and will depend on the patient’s preference and activity of the ostomy. All patients are expected to participate in all aspects of their ostomy care; if they cannot, a caregiver may be involved in the teaching (Perry et al., 2018).
Continent Ostomies
Depending on the patient, a surgical procedure may be performed to create an internal pouch to collect feces or urine, which eliminates the need for an external pouch. A continent ileostomy is made from part of the ileum and is flushed a number of times each day to clean out the effluent (Koch pouch) (Oxford Radcliff Hospitals, 2013). An ileoanal ostomy is a pouch created above the anal sphincter and is also created from a portion of the ileum (Birmingham Bowel Clinic, 2011). Two types of internal urinary diversions may be created from part of the intestine. The first is an orthotopic neobladder, where a bladder is created and placed in the body at a normal bladder position; over time, with continence training, the patient can learn to void normally. The second type is a continent urinary reservoir, where a pouch is created from part of the intestine, and a catheter is inserted a number of times during the day to remove the urine (Perry et al., 2018; United Ostomy Association of America, 2017).
Physical and Emotional Assessment and Care
Patients may have co-morbidities that affect their ability to manage their ostomy care. Conditions such as arthritis, vision changes, Parkinson’s disease, or post-stroke complications may hinder a patient’s coordination and fine motor skills needed for ostomy management. In addition, the emotional burden of coping with an ostomy may be devastating for some people and may affect their self-esteem, body image, quality of life, and ability to be intimate. It is common for a person with an ostomy to struggle with body image and altered body function. The nurse’s attitude and non-verbal responses around ostomy care can help to normalize the situation and play a significant role in helping the patient adjust to new patterns of elimination. An important element of nursing care includes care both inside and outside the acute care setting. This includes ensuring the patient has the appropriate referrals to a wound / ostomy nurse and a social worker and information about support groups, possibly including online support groups (Perry et al., 2018).
Checklist 89 reviews the steps to changing an ostomy appliance (flange and pouch).
Checklist 89: Changing an Ostomy Appliance (Flange and Pouch)
Disclaimer: Always review and follow your agency policy regarding this specific skill.
Safety considerations:
Pouching system should be changed every 4 to 7 days, depending on the patient and type of pouch.
If available, a wound care specialist or enterostomal therapist (ET) should be involved with care, preferably pre- and post-op.
Consult the wound care specialist / ET if there is skin breakdown, if there are challenges with flange adhesion, or if there are other concerns related to the pouching system.
Patients should participate in the care of their ostomy, and health care providers should promote patient and family involvement.
Encourage the patient to empty the pouch when it is one-third to one-half full of urine, flatus, or feces as they become heavy and have increased risk of spillage.
Ostomy product choices may be limited in acute care settings. Other choices are available in community retail settings. Encourage the patient / family to explore other options.
Follow all post-operative assessments for new ostomies according to agency policy.
Observe the center of the flange for evidence of leaking. Waste on the peristomal skin can cause skin breakdown. Leaking flanges must be changed immediately
Medications and diet may need adjusting for persons with new ileostomies or colostomies.
An ostomy belt may be used to help hold the ostomy pouch in place.
Factors that affect the pouching system include sweating, high heat, moist or oily skin, and physical exercise.
Always treat minor skin irritations immediately. Skin that is sore, wet, or red is difficult to seal with a flange.
Change ileostomy appliances PRIOR to eating to decrease the likelihood that a bowel movement will occur during appliance change.
Consider financial considerations of ostomy cost. Consult social services as necessary.
Discuss community supports and follow up nursing care following the hospitalization.
Steps
Additional Information
1. Perform hand hygiene.
This prevents the spread of microorganisms.
2. Gather supplies.
Supplies include flange, ostomy bag and clip, scissors, stoma measuring guide, waterproof pad, pen, adhesive remover for old flange, skin prep, stomahesive paste or powder, warm wet cloth(s) and dry cloth, non-sterile gloves,Ostomy supplies
3. Identify the patient and review the procedure. Encourage the patient to participate as much as possible, or observe and assist patient as they complete the procedure.
Proper identification complies with agency policy. Encouraging patients to participate helps them adjust to having an ostomy.
4. Create privacy. Place waterproof pad under pouch.
Attention to psychosocial needs is imperative.
The pad prevents the spilling of effluent on patient and bed sheets.
5. Apply non sterile gloves. Remove ostomy bag. Remove flange by gently pulling it toward the stoma. Support the skin with your other hand. An adhesive remover may be used.
If a rod is in situ, do not remove.
Measure and empty contents. Place old pouching system in garbage bag.
Removing ostomy bag from flange-001
The pouch and flange can be removed separately or as one unit.
Gentle removal helps prevent skin tears. An adhesive remover may be used to decrease skin and hair stripping.
A rod may be used during the formation of a stoma. It can only be removed by a physician or wound care nurse. If a rod is in place, it can be slid from side to side to allow the pouch to be removed.
6. Clean stoma gently by wiping with warm water. Do not use soap.
Aggressive cleaning can cause bleeding. If removing stoma adhesive paste from skin, use a dry cloth first.
Clean stoma and peristomal skin
Soaps often contain perfumes and oils, which can interfere with adhesion of the flange. Ivory soap (pure soap) is OK.
It is normal for blood to appear on the cloth, this suggests healthy blood flow to the stoma. Mucous is normal. Immediately post op the blood and mucous must be wiped from the stoma regularly to allow proper assessment of stoma colour and integrity.
7. Assess stoma and peristomal skin.
A stoma should be pink to red in colour, preferrably raised above skin level, and moist. Stomas that are flat or convex can still be healthy but they can present challenges in terms of ostomy management and directing waste into the pouch.
Assess stoma
Skin surrounding the stoma should be intact and free from wounds, rashes, or skin breakdown. Notify wound care nurse if you are concerned about the condition of the peristomal skin.
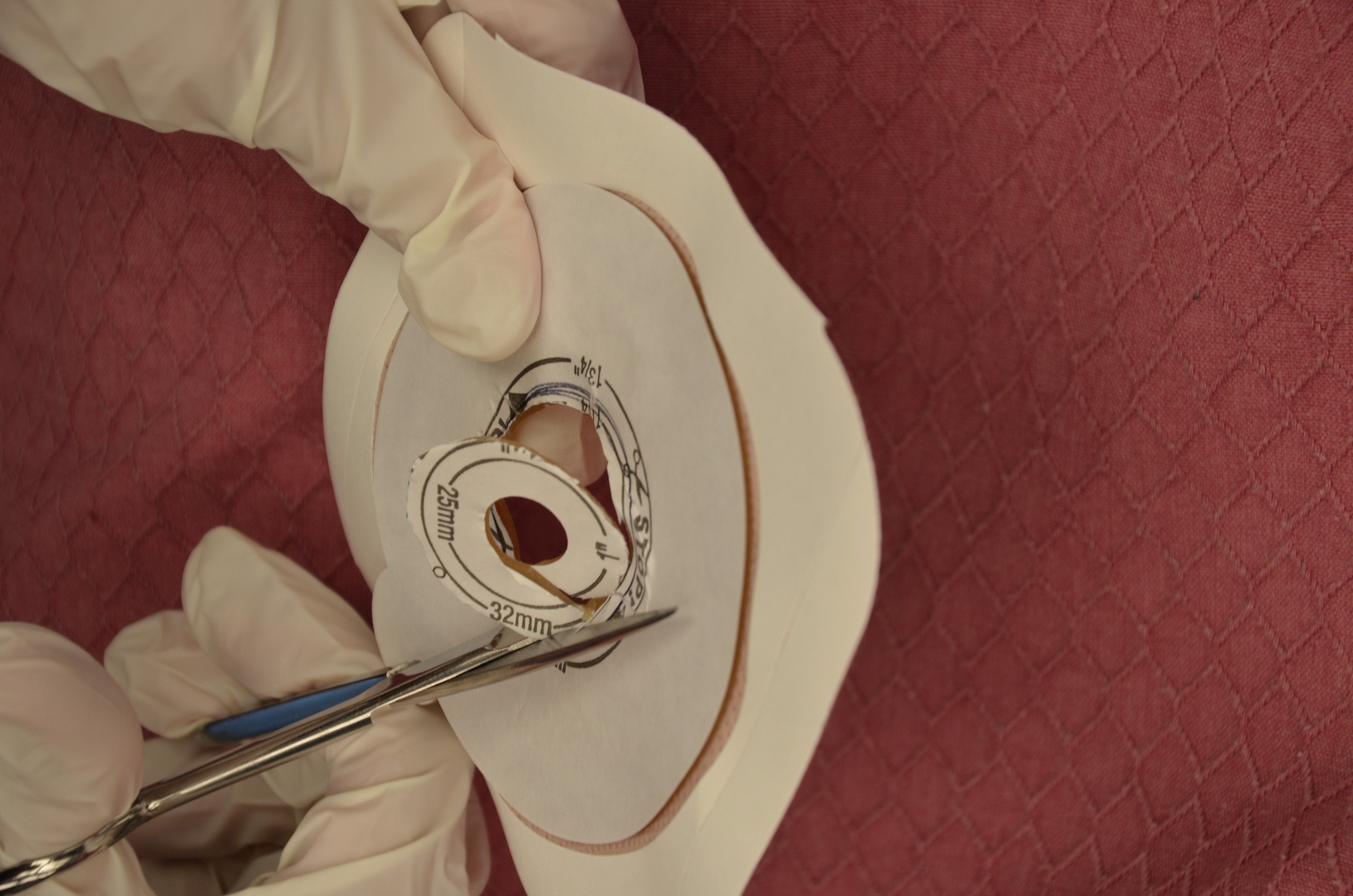
8. If the stoma is round, measure the stoma diameter using the pre-cut measuring guide (tracing template). Trace diameter of the measuring guide onto the flange, and cut on the outside of the pen marking.
If the stoma is not round, create a template (the clear plastic cover of the flange packaging works well). Trace the shape of the stoma onto this plastic. Cut out the stoma shape. Trace onto the flange and cut on the outside of the pen marking.
Some flange systems require the flange be “rolled” or “molded” from the center outward to fit the size of stoma.
Assess the flange for proper fit to the stoma.
The opening should match the stoma size. Ileostomies cannot have skin exposed between the stoma and edge of the flange. Ileostomy drainage contains enzymes that will break down intact skin causing excoriation.
Trace templateOnce size is traced onto back of flange, cut out size to fit stomaAssess flange for proper fit to stoma
Keep the measurement guide / template with patient ostomy supplies for future use.
Stomas are edematous immediately post op. Anticipate stoma size will shrink over the 6 week post-op recovery. As such the template will have to be reassessed and adjusted accordingly.
9. Prepare skin.
If adhesive remover was used to remove the flange, all residue must be removed.
Apply accessory products as required or according to agency policy.
Residue from adhesive remover will interfere with adhesion of the new flange.
Accessory products may include stomahesive paste, stomahesive powder, or products used to create a skin sealant to adhere the pouching system to skin to prevent leaking (skin prep, Eakin Seal). Wet skin will prevent the flange from adhering to the skin.
Peristomal skin prepStomahesive paste
Paste can be applied directly to the skin or to the flange just prior to applying.
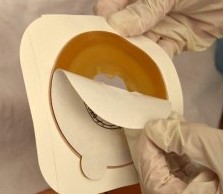
10. Remove inner backing on flange and apply flange over stoma. Leave the border tape on. Apply pressure. With the index finger press gently around the periphery of the stoma to create seal.
Then remove outer border backing and press gently to create seal.
If rod is in situ, carefully move rod back and forth but do not pull up on rod.
Remove backing from flangeApply flange around stomaWith the index finger press gently around the periphery of the stoma to create a seal
11. Apply the ostomy bag. Close the end of the bag (clip, Velcro closure, plug).
Likewise the ostomy bag can be attached to the flange prior to applying it to the body.
Secure / close the bottom of the bag according to manufacturer’s instructions.
Attach clip to bottom of bag
12. Hold palm of hand over ostomy pouch for 2 minutes to assist with appliance adhering to skin.
Some flanges are heat activated and adhere better when warmth is applied.
13. Clean up supplies, and place patient in a comfortable position. Remove garbage from patient’s room.
Removing garbage helps decrease odour.
14. Perform hand hygiene.
This minimizes the transmission of microorganisms.
15. Document procedure.
Follow agency policy for documentation. Document appearance of stoma and peristomal skin, products used, and patient’s ability to tolerate procedure and assistance with procedure.
Sample documentation: date / time: flange change complete. Stoma red, moist, warm and raised. Peristomal skin intact. Patient involved with cutting flange to correct size. Discussed frequency of flange changes and showering with an ostomy. See ostomy flowsheet — I Cee RN
Data source: BCIT, 2015; Berman & Snyder, 2016; Convatec, 2018; Perry et al., 2018; United Ostomy Association of America, 2017
Special Considerations
When patients are discharged from an acute care facility, ensure they have referrals to a community / home health nurse; that they are able to empty and change their pouch system independently or with assistance from a caregiver (this includes burping the system of excess flatus) (Ostomy Canada Society, n.d.); that they have spare supplies and know what supplies to get and where to get them (involve social services if finances are a barrier); that they know the signs and symptoms of complications and where to seek help; that they have had the necessary dietitian referral and information, particularly related to ileostomy dietary considerations (Registered Nurses Association of Ontario, 2019); that they know about showering or bathing with an ostomy appliance; that they recognize peristomal skin irritation and know what to do.
A urostomy is similar to a fecal ostomy, but it is an artificial opening for the urinary system and the passing of urine to the outside of the abdominal wall through an artificially created hole called a stoma. A urostomy is created for the following reasons:
Bladder cancer
Cystectomy
Trauma or surgery
Incontinence
Painful bladder or overactive bladder
Congenital abnormalities
Conversion of continent urinary diversion to incontinent stoma
Neurological conditions and diseases
Spinal cord injury
Chronic inflammation of bladder
Interstitial cystitis
Radiation damage
Inability to manage a continent urinary diversion or a neobladder
A person with a urostomy has no voluntary control of urine, and a pouching system must be used and emptied regularly. Many patients empty their urostomy bag every two to four hours, or as often as they regularly used the bathroom prior to their surgery. Urostomy pouches (see Figure 10.19) have a drain spot at the distal end, and the pouch should be emptied when one-third full. The pouch may also be attached to a large drainage bag for overnight drainage as an attempt to minimize sleep disturbances associated with having to wake up to attend to a full pouch. People with a urostomy are more at risk for urinary tract infections (UTIs) and should be taught about the signs and symptoms of such infections (Perry et al., 2018).
Figure 10.19 Urostomy pouch. note the different opening (left side of photo)
Changing a urostomy appliance (flange and pouch) is for the most part the same as changing an ileostomy or colostomy appliance. A few considerations specific to a urostomy are outlined in Table 10.6.
Table 10.6 How Changing a Urostomy Pouch Is Different than a Colostomy / Ileostomy
Consideration
Explanation
Urine flows continually from a urostomy making it a little more challenging to ensure a good seal with the flange.
Because the kidneys continually produce urine, a urostomy continually drips urine. Wet peristomal skin interferes with flange adhesion. Solution: Place a sterile gauze on top of the stoma to absorb urine during cleansing of peristomal skin and flange preparation. Remove it immediately before application of the new flange before urine can wet the peristomal skin.
Ureteral Stents that go from the ureter(s) through the stoma opening are placed post-operatively to prevent stricture at the ureter / stoma anastamosis site.
When ureteral stents are present, sterile technique must be used when changing a urostomy appliance. Always follow agency policy.
The stents are usually removed in the hospital by the surgeon or at the first physician visit.
When present, the stents present an extra consideration when changing the flange.
Ureteral stents facilitate urine drainage from the kidney and the increase the risk for urinary tract infection.
Following principles of asepsis, place the stents on a sterile drape during flange change. This reduces risk of introducing microorganisms into the urinary tract.
Care must be taken to avoid accidental removal of the stents during removal of the old appliance and application of the new.
Feed the stents into the drainage bag through the hole in the flange.
Like ileostomies, the weight of the effluent impacts the flanges ability to remain adhered to the skin
Change urostomy flanges every 5 days.
Urine character from a urostomy / ileal conduit is normally cloudy and can be foul smelling.
Because urine passes through a piece of bowel, the character of the urine will be cloudy from mucous and likely foul smelling from the bacteria that lives in the ileal conduit.
Without a bladder, signs and symptoms of urinary tract infection might be different than anticipated
Cloudy, foul smelling urine is no longer a potential symptom of urinary tract infection. Without a bladder, urgency and frequency are no longer possible. Assess for fever, changes to urine character (changes from the new norm), flank pain.
Encourage hydration by drinking at least 2 litres of fluid per day (unless contraindicated).
Needing to frequently empty a urostomy pouch can interfere with sleep.
Use a nighttime drainage bag attached to the pouch. When using a large urine drainage bag, the anti-reflux valve incorporated into the bag should prevent backup of urine into the urostomy pouch.
Data sources: BCIT, 2015; Perry et al., 2018; United Ostomy Association of America, 2017
What dietary or medication changes might be considered for a patient who has a new ileostomy and no longer has a small bowel?
A patient with a new colostomy refuses to look at his stoma or participate in changing the pouching system. What are some suggestions to help your patient adjust to the stoma?














{kind=link}
.png){kind=link}
{kind=link}