Chapter 2. Patient Assessment
2.12 Head-to-Toe Assessment: Integument Assessment
Checklist 22 provides a guide for objective and subjective data collection in an integument assessment.
Objective DataConsider the following: |
|
Steps |
Additional Information |
|
Abnormalities in skin / sclera colour may indicate other health issues (i.e., jaundice)
 Consider causes of excessive moisture. Excess moisture may increase the patient’s risk for skin breakdown. Excessive temperature may indicate infection. Further assessment is required. |
|
Neglect of nails may suggest difficulty with managing activities of daily living.
Fungal infection of nails is common.  |
|
 
|
|
The integumentary system is our body’s first line of defense against invading organisms. Breaks in integument increase one’s risk of infection. Any concerns should be reported to the appropriate healthcare provider immediately.
  |
|
Determine the rationale for all tubes. Tubes should be secured, intact, and functioning. See Table 10.1 Guidelines for Caring for Patients with Tubes and Devices.
Dressings should be dry and intact. |
|
The character of drainage provides insight into activities within the body. |
Subjective DataAsk if they have noticed any recent changes to their skin. |
|
Focused integument assessment may also include: |
|
| Pressure Injury Risk Assessment
Braden scales for measuring risk of developing a pressure injury are widely used in North America in the adult patient population. The tool consists of six subscales: sensory perception, moisture, activity, mobility, nutrition, friction, and shear. Using each of these elements, the nurse assigns a score. Low numbers translate to high risk of pressure injury.
|
See Braden Pressure Ulcer Risk Assessment
Some agencies have guidelines about frequency of assessment and documentation using a Braden Scale. It is important for the nurse to remember that the Braden Scale is an assessment tool. The nursing process isn’t completed unless risk is addressed through preventative strategies and evaluation of outcomes. Necessary interventions to prevent and treat pressure injury should be included in the plan of care. |
| Wound Assessment | See 4.2 Wound Healing and Assessment |
Potential integument related nursing diagnoses:
|
|
| Data sources: Braden & Bergstrom, 1989; RNAO, 2016; Potter et al., 2019 | |
Critical Thinking Exercises
- Identify the six components of the Braden Scale that suggest risk of pressure injury.
- In five of those components, provide two possible preventative strategies to reduce risk of pressure injury.
Attribution:
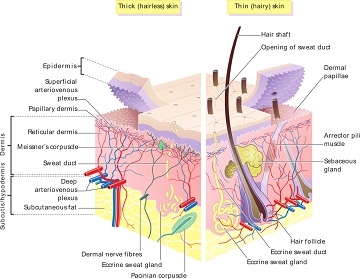
Figure 2.32 Layers of Skin by Madhero88 and M. Komorniczak is used under a Creative Commons Attribution-Share Alike 3.0 Unported license.
Figure 2.33 Jaundice Caused by Hepatitis A by CDC/Dr. Thomas F. Sellers/Emory University is in the public domain.
Figure 2.34 A Patient’s Left Foot – After Ten Weeks of Terbinafine Oral Treatment by Dandandandandandandan2014 is used under a Creative Commons Attribution-Share Alike 4.0 International license.
Figure 2.35 Thrush in a Child Who Has Taken Antibiotics by James Heilman, MD is used under a Creative Commons Attribution-Share Alike 3.0 Unported license.
Figure 2.36 Herpes Labialis by Jojo is in the public domain.
Figure 2.37 Scabies by Cixia is in the public domain.
Figure 2.38 Gangrene Toe by James Heilman, MD is used under a CC BY-SA license.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}