Chapter 2. Patient Assessment
2.7 Head-to-Toe Assessment: Chest / Respiratory Assessment
Checklist 17 provides a guide for subjective and objective data collection in a respiratory assessment.
Objective DataThe data that we can observe with our senses.
|
|
Steps |
Additional Information |
Observe the work of breathing including use of accessory muscles.
 |
Increased work of breathing may be observed through a spectrum of responses including a small amount of nasal flaring through to use of all accessory muscles. Increased work of breathing is often associated with an increased respiratory rate.
The patient may appear distressed and/or feel anxious. Likewise they may not appear distressed, depending on the severity and other comorbidities. Ability to speak may be affected. Increased work of breathing may indicate respiratory compromise and impaired oxygenation caused by things like acute airway obstruction, pulmonary edema, atelectasis, and others. Unusual findings should be followed up with a focused respiratory assessment. More resources:
|
| Expansion / Retraction of Chest Wall | The chest wall should expand and contract symmetrically. If not, consider if this is a new or pre-existing condition.
Chest expansion may be asymmetrical with conditions such as atelectasis, pneumonia, fractured ribs, pneumothorax, or hemothorax. |
| Assess respiratory rate by inconspicuously observing breathing. One way to do this is to palpate radial pulse for a full minute but use some of that time to count respirations.
Likewise, placing your hand on the patient’s chest and counting the rise / fall cycles  |
Normal respiratory rate (interpreted as respirations per minute):
If a patient’s respiratory status is stable, it may be appropriate to count respirations for 30 seconds and multiply by two to determine respiratory rate. |
Pulse Oximetry: Consists of a probe with a light-emitting diode (LED) attached to the patient’s finger, forehead, or ear. Beams of red and infrared light are emitted from the LED, and the light wavelengths are absorbed differently by the oxygenated and the deoxygenated hemoglobin (Hgb) molecules. The receiving sensor measures the amount of light absorbed by the oxygenated and deoxygenated Hgb in the arterial (pulsatile) blood. (Perry et al., 2018).
 |
The more Hgb that is saturated with oxygen, the higher the SpO2, which should normally measure above 95% oxygen saturation (SpO2) (Perry et al., 2018). |
| Use a stethoscope to auscultate breath sounds anterior and posterior for quality of air entry and any adventitious sounds. Assess bilaterally comparing one side with the other in a systematic fashion.
|
Diminished air entry may indicate atelectasis, pneumonia, hemothorax, pneumothorax, or collapsed lung.
The presence of crackles or wheezing must be further assessed, documented, and reported. If such things are affecting the patient negatively, intervention is needed. Crackles may indicated mucous related to asthma or chronic obstructive pulmonary disease (COPD), or fluid related to pulmonary edema. Wheezing may indicate bronchoconstriction related to asthma, bronchitis, or emphysema. Friction rub (creaking) may indicate inflammation related to pleurisy. The nurse should always consider what interventions they can implement independently and what interventions have been ordered by the authorized prescriber to relieve impaired oxygenation. More resources:
|
| Cough & Sputum | The nurse might observe coughing and expectorated sputum.
Reasons for coughing might include bacterial or viral infection, aspiration, or presence of sputum. Observe and ask if the cough is a concern for the patient. If sputum is present, observe or inquire about amount, colour, and consistency. Ask if sputum is normal for the patient. |

Subjective Data |
|
|
|
Focused respiratory assessment may also include: |
|
| If a chest tube is present, ensure the tube is intact and secure and that the drainage system is functioning. Auscultate chest sounds, perform a respiratory assessment including palpating for evidence of subcutaneous emphysema at and near the chest tube insertion site. See 10.6 Chest Tube Drainage Systems | |
| Arterial blood gasses (ordered by prescriber or as per agency protocol) | |
Potential respiratory related nursing diagnoses:
|
|
| Sources: Assessment Skill Checklist, 2014; Jarvis, Browne, MacDonald-Jenkins, & Luctkar-Flude, 2014; Perry, Potter, & Ostendorf, 2018; Potter et al, 2019; Stephen, Skillen, Day, & Jensen, 2012; Wilson & Giddens, 2013 | |
Critical Thinking Exercises
- A client is experiencing mild respiratory distress. Identify two important strategies to address this.
- What potential respiratory issues might the nurse anticipate for the post op patient? Identify an important nursing intervention for each.
- Identify two strategies the nurse might implement for the immobile client whose chest sounds reveal decreased air entry to the bases.
Attributions:
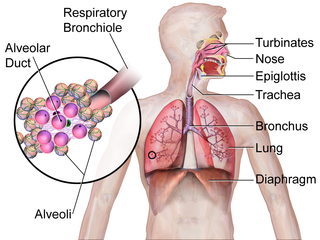
Figure 2.9 An Illustration Depicting the Respiratory System by BruceBlaus is used under a Creative Commons Attribution-Share Alike 4.0 International license.
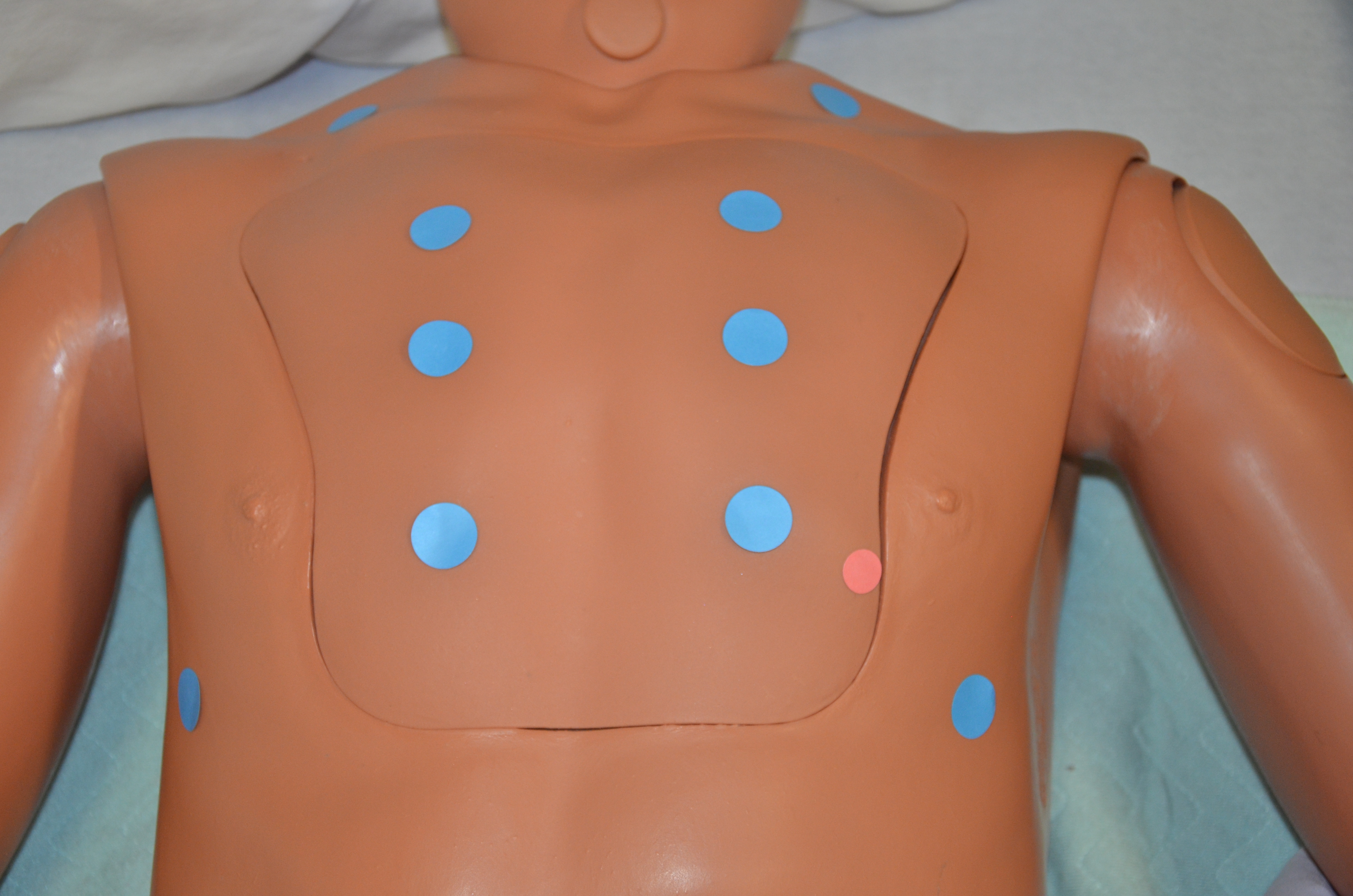
Figure 2.10 Chest Landmarks, for Radiography and Other Chest Imaging Techniques by P. Lynch is used under a Creative Commons Attribution 2.5 license.

.png){kind=link}
{kind=link}