Chapter 3. Safer Patient Handling, Positioning, Transfers and Ambulation
3.10 Assisting a Patient to Ambulate Using Assistive Devices
Immobility in hospitalized patients is known to cause functional decline and complications affecting the respiratory, cardiovascular, gastrointestinal, integumentary, musculoskeletal, and renal systems (Kalisch, Lee, & Dabney, 2013). For surgical patients, early ambulation is the most significant factor in preventing complications (Sanguinetti, Wild, & Fain, 2014). Lack of mobility and ambulation can be especially devastating to the older adult when the aging process causes a more rapid decline in function (Graf, 2006). Ambulation provides not only improved physical function, but also improves emotional and social well-being (Kalisch, Lee, & Dabney, 2013).
Prior to assisting a patient to ambulate, it is important to perform a patient risk assessment to determine how much assistance will be required. An assessment can evaluate a patient’s muscle strength, activity tolerance, and ability to move, as well as the need to use assistive devices or find additional help. The amount of assistance will depend on the patient’s condition, length of stay and procedure, and any previous mobility restrictions.
Before ambulating, the patient may need assistance getting to a sitting position.
Assisting Patient to the Sitting Position
Patients who have been immobile for a long period of time may experience vertigo, a sensation of dizziness, and orthostatic hypotension, a form of low blood pressure that occurs when changing position from lying down to sitting, making the patient feel dizzy, faint, or lightheaded (Potter et al., 2017). For this reason, always begin the ambulation process by sitting the patient on the side of the bed for a few minutes with legs dangling. Checklist 29 outlines the steps to positioning the patient on the side of a bed prior to ambulation (Perry et al., 2018).
Checklist 29: Assisting a Patient to a Sitting PositionDisclaimer: Always review and follow your agency policy regarding this specific skill. |
|||
Safety considerations:
|
|||
Steps |
Additional Information |
||
| 1. Check prescriber’s orders for any restrictions related to ambulation due to medical treatment or surgical procedure. | Equipment (proper footwear, gait belt, or assistive devices) must be gathered prior to ambulation. Do not leave patient sitting on the side of the bed unsupervised, as this poses a safety risk. | ||
| 2. Explain what will happen and let the patient know how they can help. | This step provides the patient with an opportunity to ask questions and help with the positioning. | ||
| 3. Lower bed and ensure brakes are applied. | This prepares the work environment. | ||
| 4. Stand facing the head of the bed at a 45-degree angle with your feet apart, with one foot in front of the other. Stand next to the waist of the patient. | Proper positioning helps prevent back injuries and provides support and balance. | ||
| 5. Have patient turn onto side, facing toward the caregiver. Assist patient to move close to the edge of the bed. | Turning, rolling, and leverage requires less work than lifting. This step prepares the patient to be moved.
 |
||
| 6. Place one hand behind patient’s shoulders, supporting the neck and vertebrae. | This provides support for the patient.
If available, use the electric bed to elevate the patient’s torso to a sitting position. |
||
| 7. On the count of three, instruct the patient to use their elbows to push up on the bed and then grasp the side rails, as you support the shoulders as the patient sits up. Shift weight from the front foot to the back foot. | Do not allow the patient to place their arms around your shoulders. This action can lead to serious back injuries. | ||
| 8. At the same time as you’re shifting your weight, gently grasp the patient’s outer thighs with your other hand and help the patient slide their feet off the bed to dangle or touch the floor. | This step helps the patient sit up and move legs off the bed at the same time.
 |
||
|
9. Bend your knees and keep back straight and neutral. |
Use of proper body mechanics helps prevent injury when handling patients. | ||
|
10. On the count of three, gently raise the patient to sitting position. Ask patient to push against bed with the arm closest to the bed, at the same time as you shift your weight from the front foot to the back foot. |
This allows the patient to help with the process and prevents injury to the healthcare provider.
 |
||
|
11. Assess patient for orthostatic hypotension or vertigo. |
If patient is not dizzy or lightheaded, the patient is safe to ambulate. If patient becomes dizzy or faint, lay patient back down on bed. |
||
|
12. Continue with mobilization procedures as required. |
Mobilization helps prevent complications and improves physical function in hospitalized patients. | ||
| Data sources: Interior Health, 2013; Perry et al., 2018; PHSA, 2010 | |||
Assisting a Patient to Ambulate
Ambulation is defined as moving a patient from one place to another (Potter et al., 2010). Once a patient is assessed as safe to ambulate, the nurse must determine if assistance from additional healthcare providers or assistive devices is required. The following checklists provide guidance in assisting to ambulate using a gait belt or transfer belt (see Checklist 30), walker (Checklist 31), crutches (Checklist 32), and a cane (Checklist 33).
Checklist 30: Assisting to Ambulate Using a Gait Belt / Transfer Belt
Disclaimer: Always review and follow your agency policy regarding this specific skill. |
|||
Safety considerations:
|
|||
Steps |
Additional Information |
||
| 1. Ensure patient does not feel dizzy or lightheaded and is tolerating the upright position.
Instruct the patient to sit on the side of the bed first, prior to ambulation. Ensure proper footwear is on patient, and let patient know how far you will be ambulating. Check physician’s orders for any activity restrictions related to treatment or surgical procedures. |
Proper footwear is non-slip or slip-resistant footwear. Socks are not considered proper footwear. Proper footwear is essential in preventing accidental falls.
 |
||
| 2. Explain to the patient what will happen and what they can do to help.
Apply gait belt snugly around the patient’s waist. |
   |
||
| 3. Stand in front of the patient, grasping each side of the gait belt, keeping back straight and knees bent. | The patient must be cooperative and predictable, able to bear weight on own legs, and have good trunk control. | ||
| 4. While holding the belt, gently rock back and forth three times. On the third time, assist the patient to rise into a standing position. | This action provides momentum to help patient into a standing position. Count out loud so the patient knows what to expect.
  |
||
| 5. Once patient is standing and feels stable, move to the unaffected side and grasp the gait belt in the middle of the back. With the other hand, hold the patient’s hand closest to you. | Standing to the side of the patient provides assistance without blocking the patient. | ||
| 6. Before ambulating ask the patient if they feel dizzy or lightheaded. If they do, sit patient back down on the bed.
If patient feels stable, begin walking, matching your steps to the patient’s. Instruct patient to look ahead and lift each foot off the ground. |
Risk assessment is ongoing.
Walk only as far as the patient can tolerate without feeling dizzy or weak.
|
||
| 7. To help a patient back to bed, have patient stand with back of knees touching the bed. Grasp the gait belt and help patient into a sitting position, keeping your back straight and knees bent. | Allowing a patient to rest after ambulation helps prevent fatigue.
Short frequent walks help to build stamina. |
||
| 8. When patient is finished ambulating, remove gait belt, and settle patient into bed or a chair. | This provides a safe place for the patient to rest.
|
||
| 9. Leave the patient in a safe place. If in bed, place the bed in lowest position, raise side rails as required, and ensure call bell is within reach. Perform hand hygiene. | Placing bed and side rails in a safe position reduces the likelihood of injury to patient. Proper placement of call bell facilitates patient’s ability to ask for assistance.
 Hand hygiene reduces the spread of microorganisms. |
||
| 10. Document patient’s ability to tolerate ambulation and type of assistance required. Update the care plan as required. | This provides a baseline of patient’s abilities and promotes clear communication between health care providers. | ||
| Data sources: Interior Health, 2013; Perry et al., 2018; PHSA, 2010 | |||

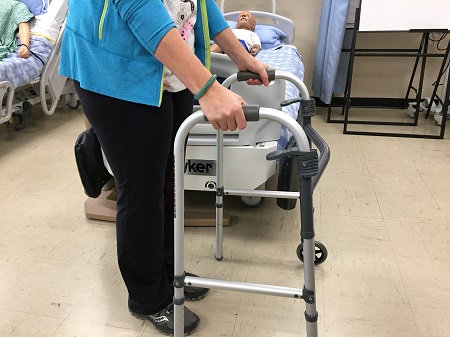
Checklist 31: Ambulating with a Walker Disclaimer: Always review and follow your agency policy regarding this specific skill. |
|||
Safety considerations:
|
|||
Steps |
Additional Information |
||
| 1. Ensure proper footwear is on the patient, and let the patient know how far you will be ambulating. Proper footwear is non-slip or slip-resistant footwear. If in acute care, check prescriber’s orders for any activity restrictions related to treatment or surgical procedures. | Proper footwear is essential to prevent accidental falls.
 |
||
| 2. Measure client for walker height. |
 The top of the walker should line up with the crease on the inside of the wrists when one is standing. Elbows should flex 15-30 degrees when standing inside the walker with hands on the hand grips. |
||
| 3. Explain and demonstrate how to walk with a walker. |
 |
||
| 4. From a sitting position, instruct patient to push up from the chair’s armrest to a standing position. | Do not use the walker to pull oneself up. It is not stable and could result in injury.
 Apply gait belt if required for additional support. |
||
| 5. Firmly grip both sides of the walker.
Move the walker forward a short distance. |
The base of the walker provides a broad base of support.
Once patient is standing and feels stable, move to the unaffected side. If using a gait belt, grasp the belt in the middle of the patient’s back. |
||
| 6. Step forward with the injured or weak leg first, taking weight through one’s hands.
Then step with the stronger leg. |
Do not step forward if all four feet of the walker are not in contact with the floor.
Walker – weak leg – strong leg. Keep feet within the walker’s boundaries. Advise the patient to look forward not down at the floor. |
||
| 7. To turn: Advise to take small steps, moving the walker and then the legs. | Avoid twisting the knee joint when turning. Walking in a large circle may be necessary. | ||
| Data sources: Cleveland Clinic, 2018a; Perry et al., 2018 | |||
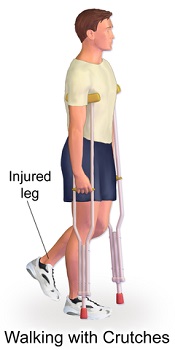
Checklist 32: Ambulating with Crutches
Disclaimer: Always review and follow your agency policy regarding this specific skill. |
|||||
Safety considerations:
|
|||||
Steps |
Additional Information |
||||
| 1. Ensure proper footwear is on the patient, and let the patient know how far you will be ambulating. Proper footwear is non-slip or slip-resistant footwear. If in acute care, check prescriber’s orders for any activity restrictions related to treatment or surgical procedures. | Proper footwear is essential to prevent accidental falls. An informed patient is part of delivering safe patient care.
|
||||
| 2. Ensure crutch height is correct. | Axilla height crutches: When standing, the there should be two to three finger widths from the axilla to the top of the crutch. The height of the hand grip will be adjusted to allow the elbow to be flexed 15 to 30 degrees or to the wrist crease. There are different crutch walking techniques that depend on the patient’s ability to bear weight.
Forearm crutches: The elbows should be flexed 15 to 30 degrees when holding the hand grips. The forearms should be supported roughly mid-point between the wrist and elbow. |
||||
| 3. Explain and demonstrate how to walk with crutches. | An informed patient may result in reduced risk of falls. | ||||
| 4. From a sitting position, advise the patient to push up from the chair’s armrest to a standing position. Stand to gain balance. Advise the patient to not lean on the underarm supports. | The patient should be cooperative and predictable, able to bear weight on own legs, and to have good trunk control. Apply gait belt if required for additional support.
Pressure on the axilla can cause damage to tissues and nerves. |
||||
| 5 a. Advise patient accordingly:
Ambulation method #1:
|
Bear in mind any weight bearing limitations. | ||||
5 b. Ambulation method #2:
|
Ambulation method #2 requires good balance and trunk strength. | ||||
6 a. Ascending stairs:
|
Strong leg – weak leg – crutches.
Use of the hand rail may be helpful. |
||||
6 b. Descending stairs:
|
Crutches – weak leg – strong leg.
Use of the hand rail may be helpful. |
||||
| Data sources: Cleveland Clinic, 2018b; Perry et al., 2018 | |||||

Checklist 33: Ambulating with a Cane Disclaimer: Always review and follow your agency policy regarding this specific skill. |
|||
Safety considerations:
|
|||
Steps |
Additional Information |
||
Proper footwear is non-slip or slip-resistant footwear.
|
Proper footwear is essential to prevent accidental falls. An informed patient is part of delivering safe patient care.
|
||
| 2. Ensure cane height is correct. | Cane height is the length from the greater trochanter to the floor. Allow 15 to 30 degree flexion at the elbow. | ||
| 3. Explain and demonstrate how to walk with crutches. | An informed patient may result in reduced risk of falls. | ||
| 4. Encourage the patient to get to a standing position. | Quad cane: Push up from the armrest of the chair to standing position. Grasp cane and establish balance.
 Standard cane: Hold the cane handle in one hand. Push up from the armrest to standing position. Establish balance. |
||
| 5. Advise the patient to move the cane forward a short distance. | Cane position is forward and slightly to the side when ambulating. | ||
| 6. Step forward with injured / weak leg. Put weight onto the cane handle. Then step with the strong leg. | Cane – weak leg – strong leg. | ||
7 a. Ascending stairs:
|
Strong leg – weak leg – cane.
Quad canes may have to be turned sideways to fit on a stair. Use of hand rail may help improve balance. |
||
7 b. Descending stairs:
|
|||
| Data sources: Cleveland Clinic, 2018c; Perry et al., 2018 | |||
Critical Thinking Exercises
- A 90-year-old patient is required to ambulate. He had a total hip arthroplasty and is post-operative day 2 (POD 3). What risk factors should be considered prior to ambulating an elderly patient who has been immobile after hip surgery?
- Does ambulation require an order from a prescriber?
- What should you do if a patient feels dizzy or lightheaded before ambulation?
Attributions
Figure 3.8 Walker by rawpixel.com is free of copyright.
Figure 3.9 Standing with support of a walker by author is licensed under a Creative Commons Attribution 4.0 International License.
Figure 3.10 Preparing to move from chair to walker by author is licensed under a Creative Commons Attribution 4.0 International License.
Figure 3.11 Teenage boy on crutches with walking boot by Pagemaker787 is used under a Creative Commons Attribution-Share Alike 4.0 International license.
Figure 3.12 An illustration depicting walking on crutches by BruceBlaus is used under a Creative Commons Attribution-Share Alike 4.0 International license.
Figure 3.13 An illustration depicting different cane types by BruceBlaus is used under a Creative Commons Attribution-Share Alike 4.0 International license.
Figure 3.14 Cane height by author is licensed under a Creative Commons Attribution 4.0 International License.

{kind=link}
{kind=link}
{kind=link}