Chapter 5. Oxygen Therapy
5.5 Oxygen Therapy Systems
Tissue oxygenation is dependent on optimal or adequate delivery of oxygen to the tissues. Increasing the concentration of inhaled oxygen is an effective method of increasing the partial pressure of oxygen in the blood and correcting hypoxemia. Simply stated, oxygen therapy is a means to provide oxygen according to target saturation rates (as per physician orders or hospital protocol) to achieve normal or near normal oxygen saturation levels for acute and chronically ill patients (O’Driscoll et al., 2008). Those administering oxygen must monitor the patient to keep the saturation levels within the required target range. Oxygen should be reduced or discontinued in stable patients with satisfactory oxygen saturation levels (Perry et al., 2014).
Hypoxemia or hypoxia is a medical emergency and should be treated promptly. Failure to initiate oxygen therapy can result in serious harm to the patient. The essence of oxygen therapy is to provide oxygen according to target saturation rates, and to monitor the saturation rate to keep it within target range. The target range (SpO2) for a normal adult is 92% to 98%. For patients with COPD, the target SpO2 range is 88% to 92% (Alberta Health Services, 2015; Kane et al., 2013; O’Driscoll et al., 2008).
Although all medications given in the hospital require a prescription, oxygen therapy may be initiated without a physician order in emergency situations (BCCNP, 2019). Most hospitals will have a protocol in place to allow health care providers to apply oxygen in emergency situations. The health care provider administering oxygen is responsible for monitoring the patient response and keeping the oxygen saturation levels within the target range.
The most common reasons for initiating oxygen therapy include acute hypoxemia related to pneumonia, shock, asthma, heart failure, pulmonary embolus, myocardial infarction resulting in hypoxemia, post-operative states, pneumothorax, and abnormalities in the quality and quantity of hemoglobin. There are no contraindications to oxygen therapy if indications for therapy are present (Kane et al., 2013).
Oxygen Delivery Systems
There is a wide variety of devices available to provide oxygen support. Delivery systems are classified as low-flow or high-flow equipment, which provide an uncontrolled or controlled amount of supplemental oxygen to the patient (O’Driscoll et al., 2008). Selection should be based on preventing and treating hypoxemia and preventing complications of hyper-oxygenation. Factors such as how much oxygen is required, the presence of underlying respiratory disease, age, the environment (at home or in the hospital), the presence of an artificial airway, the need for humidity, a tolerance or a compliance problem, or a need for consistent and accurate oxygen must be considered to select the correct oxygen delivery device (O’Driscoll et al., 2008). Table 5.3 lists types of oxygen equipment.
Table 5.3 Types of Oxygen Equipment |
|||||||
Types of Oxygen Equipment |
Additional Information |
||||||
| Nasal-cannula (low-flow system) | Nasal cannula consists of a small bore tube connected to two short prongs that are inserted into the nares to supply oxygen directly from a flow meter or through humidified air to the patient. It is used for short- or long-term therapy (i.e., COPD patients), and is best used with stable patients who require low amounts of oxygen.
Advantages: Can provide 24% to 40% O2 (oxygen) concentration. Most common type of oxygen equipment. Can deliver O2 at 1 to 6 litres per minute (L/min). It is convenient as patient can talk and eat while receiving oxygen. May be drying to nares if level is above 4 L/min. Easy to use, low cost, and disposable. Limitations: Easily dislodged, not as effective is a patient is a mouth breather or has blocked nostrils or a deviated septum or polyps. Nasal dryness can occur   |
||||||
| Simple face mask (low-flow system) | A mask fits over the mouth and nose of the patient and consists of exhalation ports (holes on the side of the mask) through which the patient exhales CO2 (carbon dioxide). These holes should always remain open. The mask is held in place by an elastic around the back of the head, and it has a metal piece to shape over the nose to allow for a better mask fit for the patient. Humidified air may be attached if concentrations are drying for the patient.
Advantages: Can provide 40% to 60% O2 concentration. Flow meter should be set to deliver O2 at 6 to 10 L/min. Used to provide moderate oxygen concentrations. Efficiency depends on how well mask fits and the patient’s respiratory demands. Readily available on most hospital units. Provides higher oxygen for patients. Disadvantages: Difficult to eat with mask on. Mask may be confining for some patients, who may feel claustrophobic with the mask on. Note: exhalation ports / holes/ vents on the sides of the mask must be open to allow for gas exchange  |
||||||
| Non re-breather mask (high-flow system) | Consists of a simple mask and a small reservoir bag attached to the oxygen tubing connecting to the flow meter. With a re-breather mask, there is no re-breathing of exhaled air. It has a series of one-way valves between the mask and the bag and the covers on the exhalation ports. On inspiration, the patient only breathes in from the reservoir bag; on exhalation, gases are prevented from flowing into the reservoir bag and are directed out through the exhalation ports.
Advantages: With a good fit, the mask can deliver between 60% and 80% FiO2 (fraction of inspired oxygen). The flow meter should be set to deliver O2 at 10 to 15 L/min. Flow rate must be high enough to ensure that the reservoir bag remains partially inflated during inspiration. 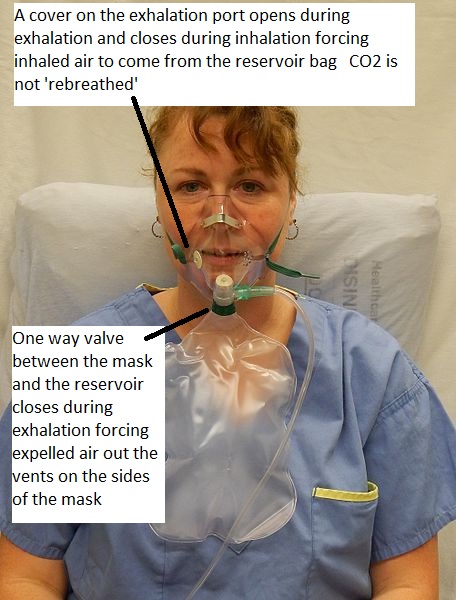 Disadvantages: These masks have a risk of suffocation if the gas flow is interrupted. The bag should never totally deflate. The patient should never be left alone unless the one-way valves on the exhalation ports are removed. This equipment is used by respiratory therapists for specific short-term, high oxygen requirements such as pre-intubation and patient transport. They are not available on general wards due to: 1. the risk of suffocation, 2. the chance of hyper-oxygenation, and 3. their possible lack of humidity. The mask also requires a tight seal and may be hot and confining for the patient. The mask will interfere with talking and eating. |
||||||
| Face tent (low-flow system) | The mask covers the nose and mouth and does not create a seal around the nose.
Advantages: Can provide 28% to 100% O2 Flow meter should be set to deliver O2 at a minimum of 15 L/min. Face tents are used to provide a controlled concentration of oxygen and increase moisture for patients who have facial burn or a broken nose, or who are are claustrophobic. Disadvantages: It is difficult to achieve high levels of oxygenation with this mask…but sometimes this is the only option  |
||||||
| Venturi mask (high-flow system) | High-flow system consisting of a bottle of sterile water, corrugated tubing, a drainage bag, air/oxygen ratio nebulizer system, and a mask that works with the corrugated tubing. The mask may be an aerosol face mask, tracheostomy mask, a T-piece, or a face tent. The key is that the flow of oxygen exceeds the peak inspiratory flow rate of the patient, and there is little possibility for the patient to breathe in air from the room
Advantages: The system can provide 24% to 60% O2 at 4 to 12 L/min. Delivers a more precise level of oxygen by controlling the specific amounts of oxygen delivered. The port on the corrugated tubing (base of the mask) sets the oxygen concentration. Delivers humidified oxygen for patient comfort. It does not dry mucous membranes. Disadvantages: The mask may be hot and confining for some patients, and it interferes with talking and eating. Need a properly fitting mask. Nurses may be asked to set up a high-flow system. In other instances, respiratory therapists may be responsible for regulating and monitoring the high-flow systems.  |
||||||
| Oxygen concentrator aka nebulizer / humidifier (high flow system) | Concentrates oxygen from the wall source up to 100%. Delivers humidified oxygen for patient comfort and to reduce risk of drying out mucous membranes.
 |
||||||
| High flow oxygen therapy (HFT) | Oxygen delivery system that has the ability to deliver:
|
||||||
| Data source: Perry et al., 2018; Vancouver Coastal Health Authority, 2015; Fisher & Paykel, 2018 | |||||||
Special considerations:
- Review the protocol in your agency prior to initiating any high-flow oxygen systems, and consult your respiratory therapist.
- In general, nasal prongs and a simple face mask (low-flow oxygen equipment) may be applied by a health care provider. All other oxygen equipment (high-flow systems) must be set up and applied by a respiratory therapist.
- For patients with asthma, medicated nebulizer treatments should use oxygen at a rate greater than 6 L/min. The patient should be changed back to previous oxygen equipment when treatment is complete.
- Oxygenation is reduced in the supine position. Hypoxic patients should be placed in an upright position unless contraindicated (e.g., if they have spinal injuries or loss of consciousness).
- In general, for most patients with COPD, target saturation is 88% to 92%. Although the risk is extremely low, it is important to recognize COPD patients are at risk for hypercapnic respiratory failure.
- Check the function of the equipment and complete a respiratory assessment at least once each shift for low-flow oxygen and more often for high-flow oxygen.
- In acutely ill patients, oxygen saturation levels may require additional ABGs to regulate and manage oxygen therapy.
- Oxygen saturation levels and delivery equipment should be documented on the patient’s chart.
Increasing Oxygen in the Lungs
The use of oxygen delivery systems is only one component to increasing oxygen to the alveolar capillary bed to allow for optimal oxygenation to the tissues. Additional methods to increase oxygen saturation levels in the body include (Perry et al., 2014):
- Maintaining satisfactory airway
- Optimizing oxygen-carrying capacities (hemoglobin levels)
- Reversing any respiratory depressants
- Using invasive or non-invasive ventilation when necessary
- Treating airflow obstruction with bronchodilators and sputum-clearing techniques
- Treating pulmonary edema as required
Critical Thinking Exercises
- Explain the difference between low- and high-flow oxygen delivery systems.
- The reservoir bag on a non re-breather mask must always be kept partially inflated. Why?
- Why are non re-breather masks not available on the general nursing units?
Attributions
Figure 5.1 A non rebreather by James Heilman, MD is used under a Creative Commons Attribution-Share Alike 4.0 International license.
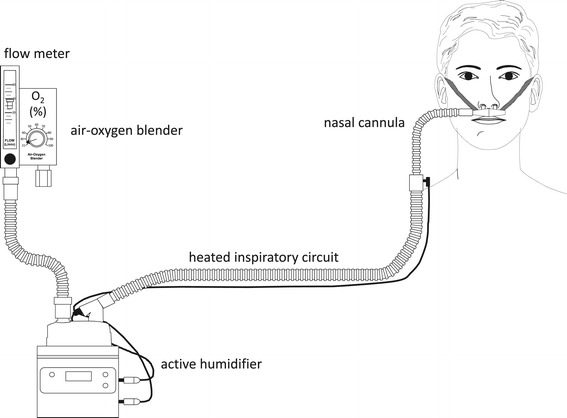
Figure 5.3 Principle setup of high-flow nasal cannula oxygen therapy by Nishimura, Masaji is used under a CC-BY 4.0 license

{kind=link}