Upper Limb
Bones
The Clavicle:
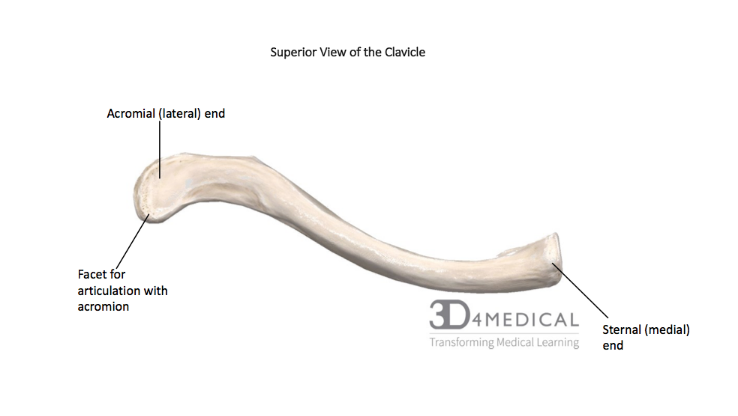
The clavicle or collarbone is termed a “S” shaped morphological structure due to its convex anterior shape (medial two thirds) and concave posterior shape (lateral one third). This bone is located on either sides of the manubrium or breastbone. The clavicle has a sternal end where the manubrium articulates with the clavicle, and acromial end where it articulates with the acromion of the scapula; a boney projection extending from the scapula. The clavicles are imperative, as they are structural components of the pectoral gridle and the bony connection of the pectoral girdle with the axial skeleton. The pectoral gridle consists of the clavicle, scapula and, proximal end of the humerus on both the right and left side of the upper body. The clavicle has various bony and anatomical features associated which can aid and guide an individual in siding the clavicle. The medial end, as already discussed, is the sternal end which articulates with the clavicular notch of the manubrium. Thus, the association between the sternal end of the clavicle and the manubrium can be defined as the sternoclavicular joint (further discussion and information of various types of joints and ligaments can be found within the joints and ligaments section). Moving away front the midline, the most lateral end of the clavicle is the acrominal end which articulates with the acromion of the scapula and furthermore, where the acromioclavicular joint can be located. The lateral end of the clavicle can be morphologically described as flat or broad in comparison to the medial end which is more pyramid shaped.
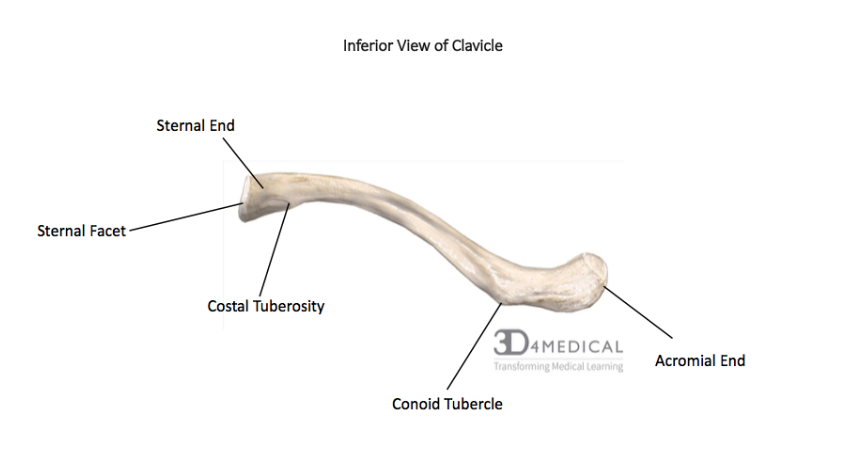
On the inferior aspect of the clavicle, there are multiple indentations. One of the indentations is an attachment site for the costoclavicular ligament and provides an attachment site for the clavicles and the first ribs. Other grooves and indentations are necessary for not only stabilization of the sternoclavicular joint, but also providing an attachment site for the subclavius muscle. The conoid tubercle can be found on the lateral aspect allowing and solidifying the connection between the clavicle and scapula via the conoid ligament. The trapezoid line is an attachment site for a ligament referred to as the trapezoid ligament, which aids in solidifying the articulation between the scapula and the clavicle. The most lateral feature on the clavicle is the articular facet which connects the clavicle to the acromion of the scapula.
The Scapula:
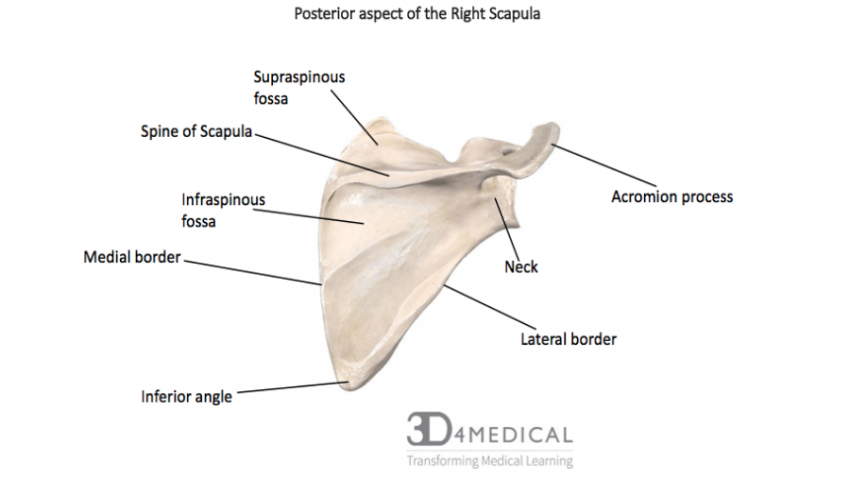
Commonly known as the shoulder blade, this triangle shaped bone can be located on the superior, posterior aspect which sits or “glides” along the thoracic cage. To allows such movements, when observed at a lateral angle the posterior face of the scapula can be described slightly convex, which allows smooth articulation with the convex structures beneath the thoracic wall. In general, the morphological structure of the bone is quite unique. This is due to various muscle attachments on the borders of the scapula and thus, is why the borders of the scapula are thicker in comparison to the body of the bone, which is thin and fragile. These borders, as already discussed, have anatomical landmarks and their nomenclature is associated with its orientation and position found within body. Beginning in the midline, the border that neighbours this region is called the medial or vertebral border (can also be termed the paravertebral border) and thus, the border that is found further from the midline is called the lateral or axillary border (due to its orientation near the axilla, commonly called the armpit). Moving to the uppermost region of the scapula, the superior border can be landmarked.
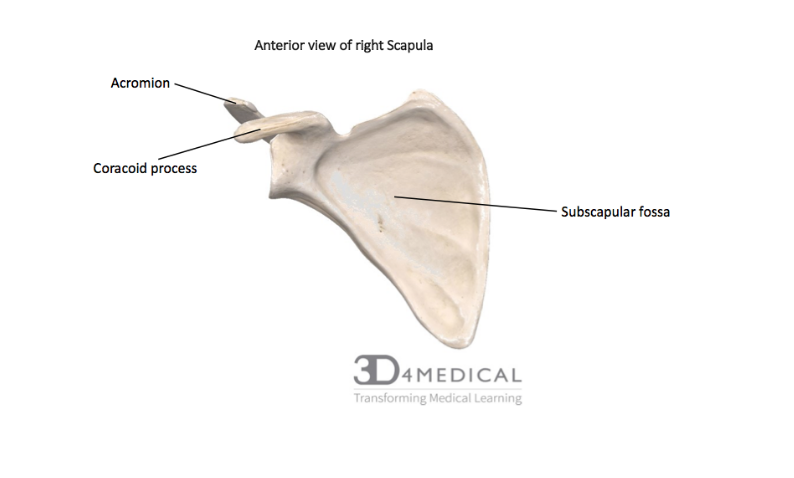
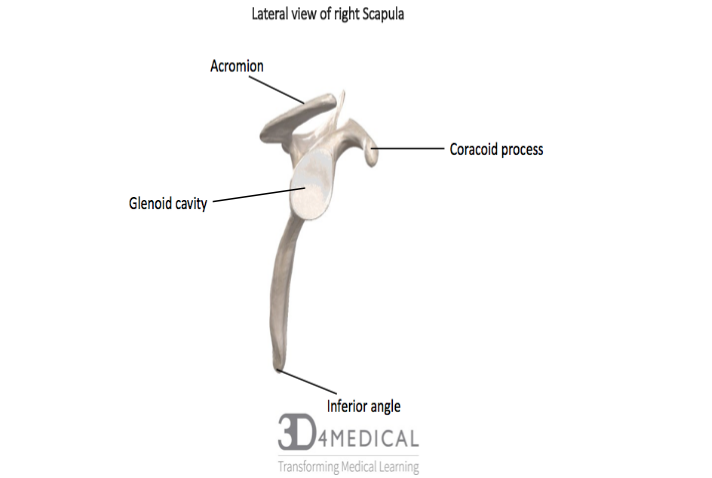
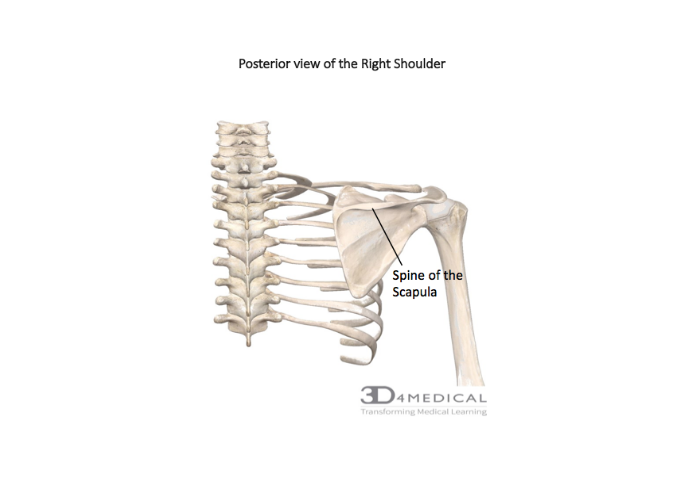
When these borders meet, they form scapular angles. The junction between the superior and the medial border forms the superior angle whereas, the medial and lateral borders come together to form the inferior angle. Finally, the remaining angle found on the scapula is the lateral angle, formed by the lateral and superior borders. We can now move onto identifiable features which allows the scapula to produce such movements such as circumduction, abduction, adduction, flexion and extension. The feature that is responsible for such actions is defined as the glenoid cavity or glenoid fossa. Another identifiable marker of the scapula is the spine of the scapula. This large, boney projection can be found on the posterior face of the scapula and is the dividing marker that separates the suprasoinatus fossa and the infraspinatus fossa. These fossas or shallow depressions are imperative to the musculature of this region. If one laterally follows the scapular spine, the acromion of the scapula can be identified. The word acromion originates from the Greek terms “akros” which is translates to the highest point and “omos” which translates to shoulder. Furthermore, the acromion contains a facet which is articulating with the clavicle at the acromioclavicular joint previously mentioned. Moving on to the anterior face of the scapula, the most definitive feature is the subscapularis fossa, which allows commorancy for the subscapularis muscle which will be discussed later in the muscular anatomy section. To conclude this section, the most anterior projection found on the scapula is the coracoid process. This boney projection originates on the superior border and projects anteriorly which acts as a muscle attachment site.
The Proximal Humerus:
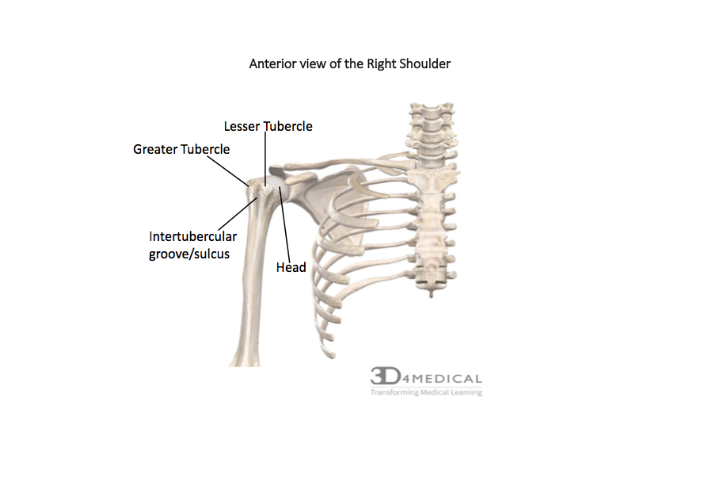
The proximal humerus is the terminating boundary of the pectoral gridle but unfortunately, with that being said, in depth discussion and analysis will not be discussed in this section. This region contains the top of the humerus, more specifically, the humeral head which articulates with the glenoid cavity; this articulation creates the glenohumeral joint. Moving distally away from he head of the humerus, the next feature in this region is the anatomical neck. This portion lies directly inferiorly to the head but also neighbours two vital muscle attachment sites which are the greater and lesser tubercles (also called major and minor tubercles along with greater and lesser tuberosities). These muscle attachments, especially the greater tubercle, projects laterally relative to the humerus and posteriorly relative to the lesser tubercle. The lesser tubercle, in comparison to the greater tubercle, projects medially and anteriorly. One last feature that will be discussed in this section is the intertubercular groove or sulcus. This feature separates or divides the greater and lesser tubercle and is another site for muscle attachments.
The Arm:
The brachium (Bra-KEY-um) or arm, refers to the upper limb which consists of only the humerus (Hu-me-RUS). The brachium radiates from the glenohumeral joint to the elbow joint, connecting the proximal end of the scapula to the distal end of the radius and the ulna. This region of the upper body allows and promotes movement of the anti-brachium (the forearm) and contributes towards gross and/or fine motor dexterity within the hands. Flexion and extension along with pronation and supination are actions produced within the brachium and anti-brachium; further discussion of the musculature involved will later be discussed in the muscles section.
The Proximal Humerus:
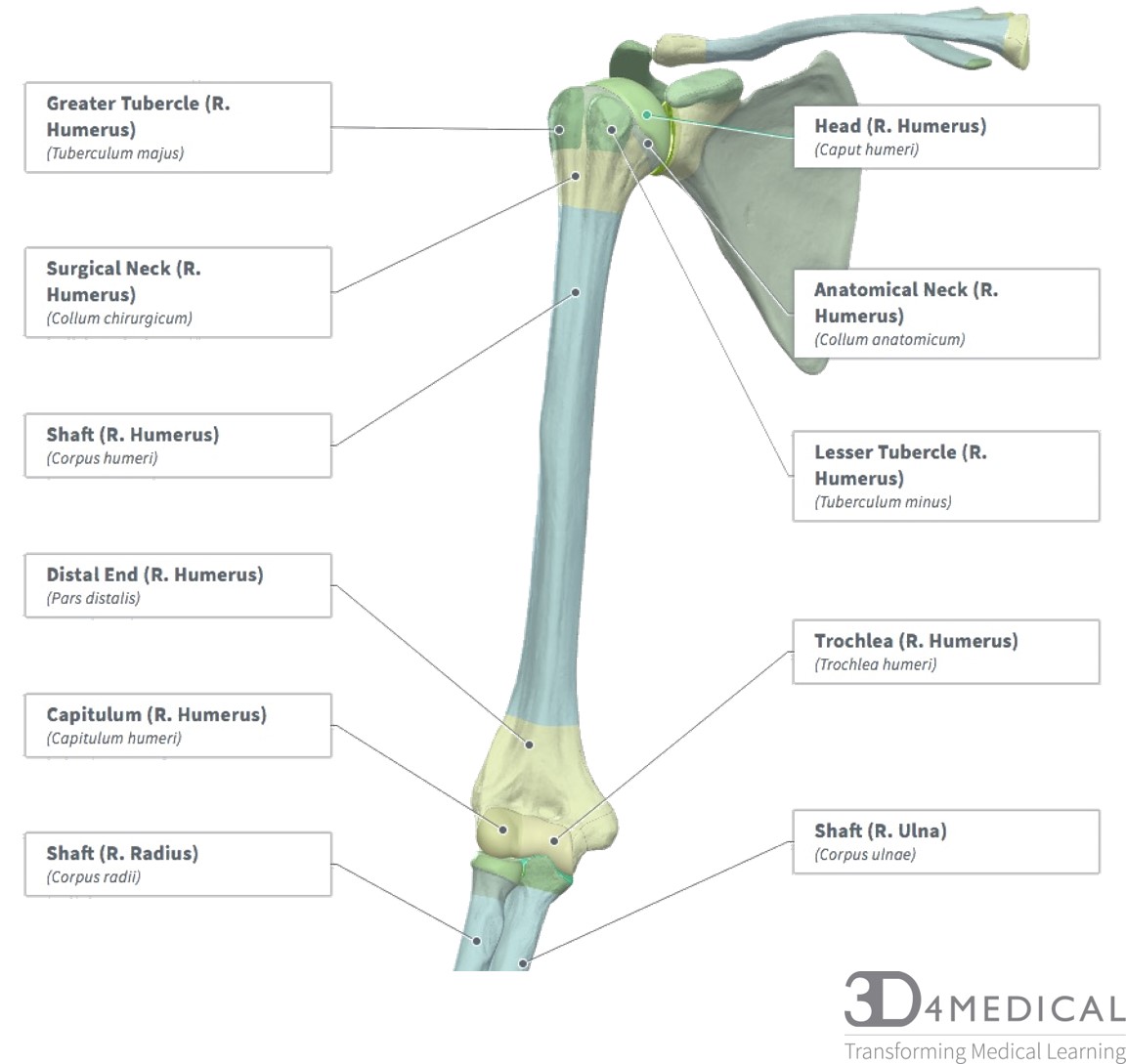
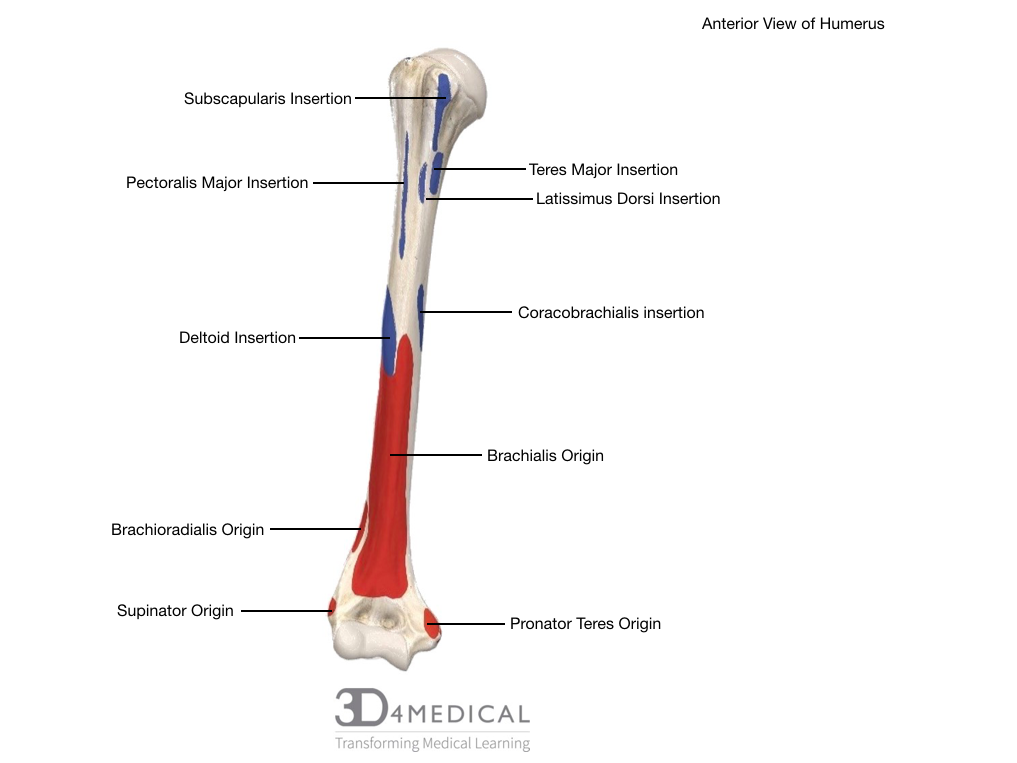
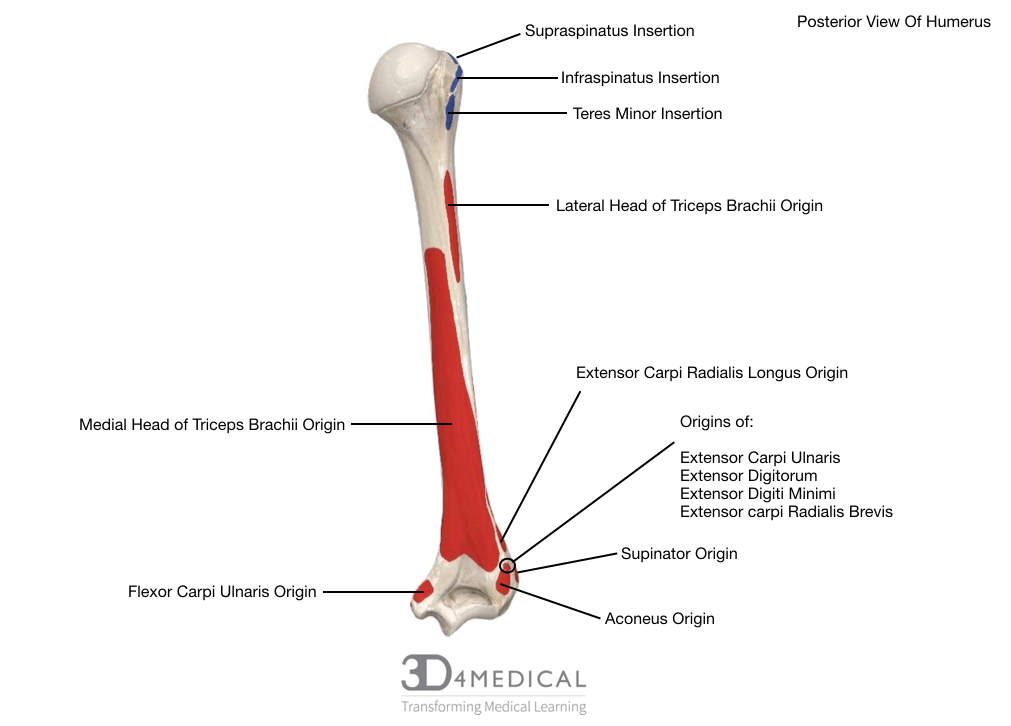
When it comes to classification and taxonomy of bones, the humerus is classified as a long bone and is the longest bone found within the upper limb. The humerus encompasses many insertion points compared to the amount of origin sites, which can be defined as picayune. Firstly, the most proximal feature of the humerus is the head of the humerus (which in bone development is defined as ephy This feature articulates with the glenoid cavity of the scapula which allows various movements and actions as previously mentioned in the paragraph above. Compared to the acetabulofemoral cavity, the glenoid cavity promotes mobility rather than stability. Because of this, injures are more prevalent in regards to the glenoid cavity than the acetabulofemoral cavity. Moving on, the humerus differs from other long bones by the factor it has two necks compared to one. The first neck, is the anatomical neck, which can be identified inferiorly from the head of the humerus. The other neck is termed the surgical neck which is inferior to the greater and lesser tubercles, but superior to the deltoid tuberosity. This feature or landmark is more commonly fractured than the anatomical neck, hence why this form of taxonomy is used. Moving on, as previously mentioned in this section, the humerus has two muscle attachments sites called the greater and lesser tubercles. The greater tubercle is the insertion point for ¾ rotator cuff muscles which are supraspinatous, infraspinatous and, teres minor; the only muscle that inserts on the lesser tubercle is the subscapularis muscle. Moving distally, a groove or indentation which separates the tubercles is defined as the intertubercular groove, or interchangeably called the bicipital groove. This groove or indentation is essential for the biceps brachii tendon to pass through and furthermore, is the insertion site for the pectoralis major, latissmus dorsi and, teres major muscle. To showcase some of the main features and surfaces of the humerus (which are not labelled in the diagram above, the image provided below highlights various origin and insertions points located on the humerus. Red indicates the origin and blue indicates the insertion landmarks).
The Distal Humerus:
The distal portion of the humerus is held responsible for hinge movements (such as flexion, extension) compared to the proximal portion of the humerus which is defined a ball and socket joint. The first feature this section is going to identify, is the cornonoid fossa and the radial fossa (lateral to the cornonoid fossa); which is found at the anterior, distal end of the humerus. The coronoid fossa articulates with the coronoid process of the ulna, and the radial fossa articulates with the radial head of the radius. Moreover, just inferior to the coronoid fossa, the capitulum and the trochlea can be identified which promote articulation with the radius and the ulna. Compared to the capitulum, the trochlea can be described as pulley shaped and articulates with the ulna via the trochlear notch. The capitulum on the other hand, is more rounded and possess a deeper, shallow depression, which allows the radial head of the radius to articulate freely. Moving to the posterior side of the humerus, the olecranon fossa can be identified which promotes movement of the “elbow”. Such movements, as previously mentioned in the beginning of the paragraph, originate when the olecranon process of the ulna moves within the olecranon fossa of the humerus. Further discussion of the olecranon, coronoid and, radial fossa’s will be discussed in the joint section as they are major factors in joint mobility.
When trying to understand the relative positioning of boney features, the condyles found at the distal end of the humerus can help orientate which side of the humerus it may belong to. The medical epicondyle is the larger, bony protuberance, which will be located medially compared to the lateral epicondyle, found laterally. Both epicondyles play a large role in muscle attachment sites as the medial epicondyle is commonly called the common flexor origin, and the lateral epicondyle is commonly called the common extensor origin. These sites are imperative for any forearm and wrist movements but due to this notion, problematic issues may arise which may lead to injury due to overuse (this will be discussed more in the clinical section under medial and lateral epicondylitis).
.
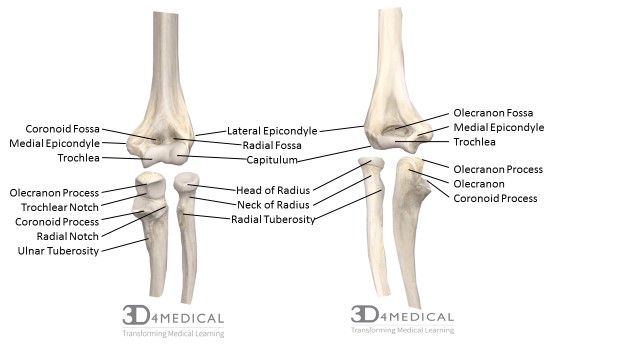
Anterior (left) and Posterior (right) view of an expanded de-articulated elbow joint of left upper limb.
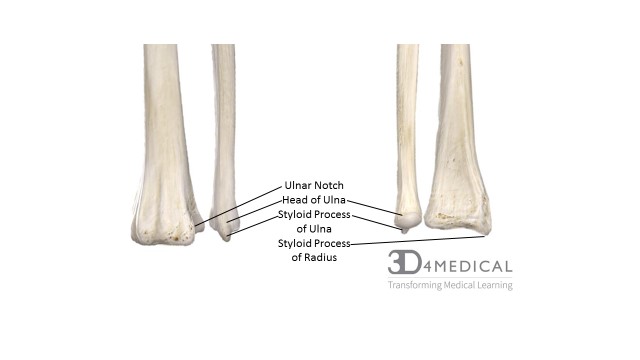
Posterior (left) and Anterior (right) de-articulated view of the distal end of the Radius and Ulna.
The Ulna:
The ulna bone is one of the two bones found within the forearm, and works alongside the radius to create various movements within. Compared to the radius, the ulna is located medially (in anatomical position) and promotes stability of the elbow joint. In the anatomical position or when relaxed, the trochlear notch locks into the trochlea of the humerus. In order to allow stability throughout such movements as flexion and extension, the coronoid process is responsible for flexion, and the olecranon is responsible for extension. Between the olecranon and the coronoid process of the ulna, the trochlear notch can be identified. Slightly inferior to the trochlear notch, the radial notch can be identified. This notch allows articulation between the ulna and the radius, which supports and enables pronation and supination of the hand. To allow such movements to occur, the radial head will twist into the radial notch meanwhile, the distal end of the radius rotates over the distal end on the ulna; therefore, creating the proximal radialulnar joint. Slightly inferior to the radial notch, the ulnar tuberosity can be landmarked which is one of two muscle attachment sites for the brachialis muscle. On the lateral surface of the ulna, and inferior to the radial notch, the supinator crest can be located. This crest forms the fossa for the coronoid process and this fossa along with the crest, are also attachment sites for the supinator muscle. Finally, the last feature of the ulna that will be discussed is the olecranon. This feature, is found on the posterior face of the ulna and is where the styloid process of the ulna can be found.
The Radius:
The radius, which is the other bone found within the forearm, which is located laterally to the ulna (in anatomical position). The morphological structure of the radial head can be described as disked like shape, which promotes significant movement; especially as it articulates with the capitulum of the humerus. The disk like shaped radial head also promotes a pivoting motion within the radial notch of the ulna. The radius, similar to the ulna, has its own tuberosity called the radial tuberosity. This tuberosity, is slightly inferior to the radial head, and is the insertion location of both heads (long head and short head) of the biceps brachii. Distally, the base of the radius can be defined as a broad surface which promotes smooth articulation with the carpal bones. Because of the morphology of the radius, during pronation and supination, the radius is the only bone that moves during such movements. The last feature that will be discussed is the styloid process of the radius. Knowing the orientation of this feature helps with siding if ever the need to occurs. The styloid process can be found on the distal, lateral end of the radius; to further state, this feature is also the attachment site of the brachioradialis tendon. Similar to the ulna which has the radial notch, the radius possesses the ulnar notch, which aids in pronation and supination movements.
Growing Pains: The Development of Carpal
Bones
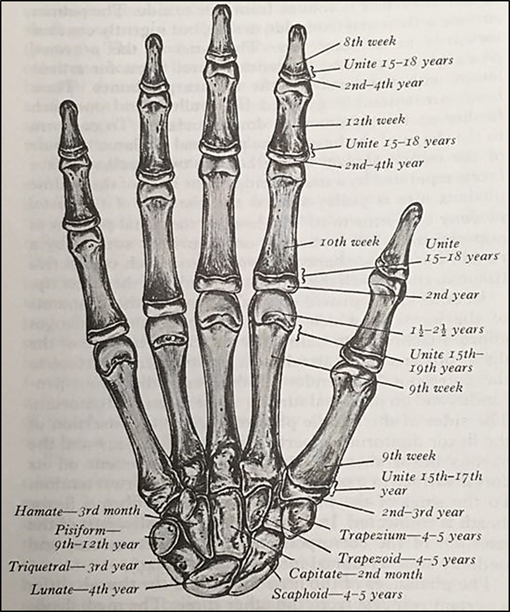
The carpal bones are usually cartilaginous at birth, and the ossification process is gradual. Ossification of the carpal bones occurs in a predictable sequence starting with the capitate and ending with the pisiform. A “handy” way to remember this sequence is to start at the capitate and then move in a counterclockwise direction on the palmar surface of the carpus. The growth status of bones can be used to assess maturation via comparison of an individual’s state of development against a standard. Skeletal age does not always match chronological age. Each individual will mature at a different and unique rate.
Comparison of the Bones of the Hands and Feet
Both the carpus and tarsus are comprised of proximal, intermediate, and distal components – i.e. carpus or tarsus, metacarpus or metatarsus, and phalanges. The digits have a wide range of motion in flexion, extension, abduction and adduction; but the hand is vastly more dynamic than the foot – hence why we are not as closely related to our primate friends. The foot is the base of the body whose components allow for a wide range of motion, support, and functionality. The powerful lever at the ankle enables complex movements such as a ballet dancer’s routine to be performed on fully pointed toes. The tarsal bones of the foot differ from the carpals mostly in size. The tarsals are much larger and stronger to provide structural support of the body’s weight. The larger nature of the tarsals restricts the motion of the foot. The hand is able to perform rotational movements (supination and pronation) whereas these movements are absent in the foot.
Carpal Bones
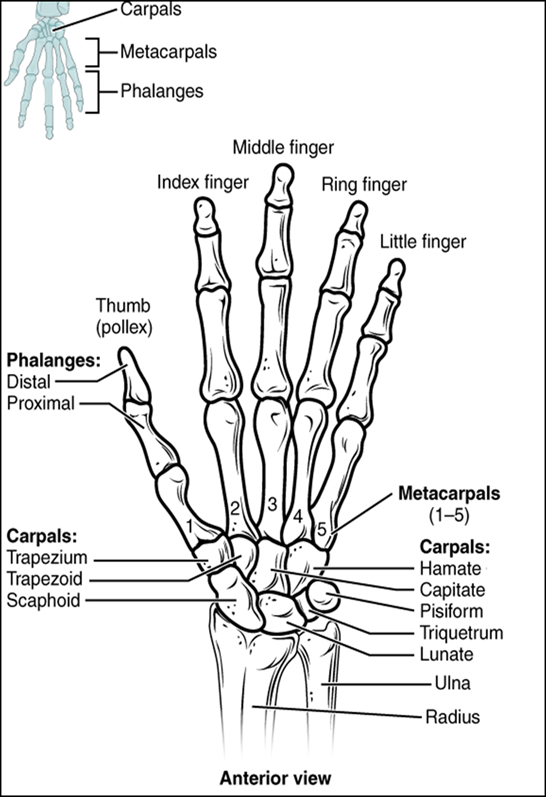
The names of each of the carpal bones come from their respective Latin or Greek roots. Each carpal bone is named for the shape they reflect. For instance, scaphoid comes from the Greek “skaphe” for boat; whereas lunate comes from the Latin “luna” for moon. In relation to the wrist, the carpal bones are noted for their location, proximal to distal, and lateral to medial. In the proximal row the bones are the: scaphoid (SKAF-oyd = boatlike), lunate (LOO-nāt = moon-shaped), triquetrum (trī-KWĒ-trum = thee-cornered), and pisiform (PIS-i-form = pea-shaped). The distal row, again from lateral to medial, are: trapezium (tra-PĒ-zē-um = four-sided figure with no parallel sides), trapezoid (TRAP-e-zoid = four-sided figure with no parallel sides), capitate (KAP-i-tāt = head-shaped), hamate (HAM-āt = hooked).
It’s a given that everyone learns differently, some can merely read a phrase and have it committed to memory, others use memory jogging techniques such as mind mapping or mnemonics.
