Lower Limb
Clinical Conditions
Burning Thigh Pain
Description:
Burning Thigh Pain is a painful condition characterized by tingling, numbness and burning pain within the outer part of the thigh. It is caused by compression to the lateral femoral cutaneous nerve, which is the nerve that provides sensation to the skin surface of the thigh. On average, this condition predominantly seems to occur in individuals between the ages of 40-60 years old.
Symptoms:
The symptoms of Burning Thigh Pain are tingling, numbness and burning pain on the outer region of the thigh. It can be a light or severe pain depending on the condition.
Treatment:
Conservative treatment measures, such as the application of ice, rest, and use of medications can help individuals with Burning Thigh Pain. The symptoms normally resolve with early treatment, or in some cases, spontaneously.
Quadriceps and Hamstring contusions:
Description:
A contusion is one of the more common injuries seen mainly in athletes competing in contact sports and results from a direct blow to the thigh. It can also be seen in accidents where anyone is involved in a direct blow to the thigh. This type of injury often goes undertreated and may result in serious complications for the athlete.
Symptoms:
Several physiological responses may occur after a deep thigh contusion including:
• Broken blood vessels resulting in bleeding (hematoma) into the injured area
• Crushed muscle tissue resulting in hip and knee dysfunction
If there is major untreated and/or unresolved bleeding deep in the muscle tissue, a serious condition known as myositis ossificans can occur. Myositis ossificans is the result of a hematoma within a muscle that calcifies rather than heals. Rather than the body healing the hematoma with fibroblasts (baby collagen fibers), the body lays down baby bone cells resulting in a bony growth deep in the muscle tissue. A myositis ossificans located deep within a quadriceps muscle can cause significant pain and disability for the athlete.
Treatment:
The general recommendation is to avoid heat during the first 24-48 hours to avoid increasing the extent of hemorrhage and edema. Once the lesion has stabilized, heat may help break up the mass of blood and tissue; however, in the literature, this has been shown to be of limited benefit. The use of crutches should be emphasized for patients with thigh contusions, as weight bearing following the thigh contusion injury may be extremely painful and may extend the damage. The knee joint should be flexed to pain tolerance in conjunction with the compression dressing. Compression gently increases tension, limiting the extent of the intramuscular hematoma. In addition, the position of flexion stretches the muscle, which increases tension and also facilitates drainage of the edematous fluid from the region. The confusion generally stabilizes by 24-48 hours, and subsequent evaluation should dictate further treatment and prognosis. Reinjury is a significant factor in prolonging disability and patients must be instructed to avoid retraumatizing the muscle.
Occupational Therapy
In the first phase of rehabilitation of a contusion, an occupational therapist may become involved by educating the patient about proper crutch use and tailoring the patient’s activities of daily living (ADL) to the immobilized limb.
Medical Issues/Complications
The index of suspicion for compartment syndrome must be high until the hemorrhage, swelling, and pain have subsided (see Miscellaneous, Medical/Legal Pitfalls).
Surgical Intervention
Surgical intervention should not be necessary in cases of contusions unless the diagnosis of compartment syndrome is considered and confirmed.
Consultations
If the diagnosis is in question or if myositis ossificans is confirmed by radiographs, orthopedic consultation can be obtained. Compartment syndrome is a surgical emergency, and an immediate consultation should be made if the diagnosis is confirmed.
Muscle strains
Description:
Muscle strains usually happen when a muscle is stretched beyond its limit, tearing the muscle fibers. They frequently occur near the point where the muscle joins the tough, fibrous connective tissue of the tendon. A similar injury occurs if there is a direct blow to the muscle. Muscle strains in the thigh can be quite painful. Once a muscle strain occurs, the muscle is vulnerable to reinjury.
Symptoms:
Symptoms of muscle strains vary but not much. Most commonly there is a sudden onset of pain, soreness and limited range of movement. More extreme muscle strains involve bruising or discoloration, swelling, could have a “knotted-up” feeling, muscle spasms and/or stiffness.
Treatment:
Rest the strained muscle and apply ice for the first few days after the injury. Anti-inflammatory medicines or acetaminophen (Tylenol) also help reduce pain and swelling. As the pain decreases, you can use heat on the muscle. Stretching and light exercises to bring blood to the injured area can also be useful.
Varicose veins
Description:
Varicose veins are enlarged, swollen, and twisting veins, often appearing blue or dark purple. They happen when faulty valves in the veins allow blood to flow in the wrong direction or to pool. More than 23 percent of all adults are thought to be affected by varicose veins.
Symptoms:
Symptoms can include aching legs, swollen ankles, and spider veins.
Treatment:
If the patient has no symptoms or discomfort and is not bothered by the sight of the varicose veins, treatment might not be necessary. However, if there are symptoms, treatment may be required to reduce pain or discomfort, address complications, such as leg ulcers, skin discoloration, or swelling. Some patients may also want treatment for cosmetic reasons – they want to get rid of the “ugly” varicose veins.
Patella-femoral syndrome
Description:
Patella-femoral syndrome is a condition characterized by pain in the front of the knee or around the patella. Happening commonly in athletes and people who participate in sport, it is also commonly referred to as “runner’s knee” or “jumper’s knee”. The pain occurs when there is abnormal tracking of the patella against the patellar surface of the femur.
Symptoms:
Patella-femoral syndrome can cause significant pain and stiffness in the knee making any activities with knee flexion and extension such as running, squatting, climbing stairs, kneeling down, and other everyday activities very painful and hard to do. Some people may also experience weakness during certain movements or even buckling at the knee. Sensations such as catching, popping, and grinding may also be experienced.
Causes & Treatment:
There are many different things that can contribute to the development of patella-femoral syndrome including misalignment of the kneecap, muscle imbalance, overuse, and vigorous training or exercises. Symptoms can often be relieved with rest or decreased activity level. In some cases, anti-inflammatory medications, physiotherapy, braces or taping, and surgery might be needed depending on severity and circumstance. Changes in exercise programs are a common and non-invasive way to help correct the body naturally.
Ilio Tibial Band Friction Syndrome
Description:
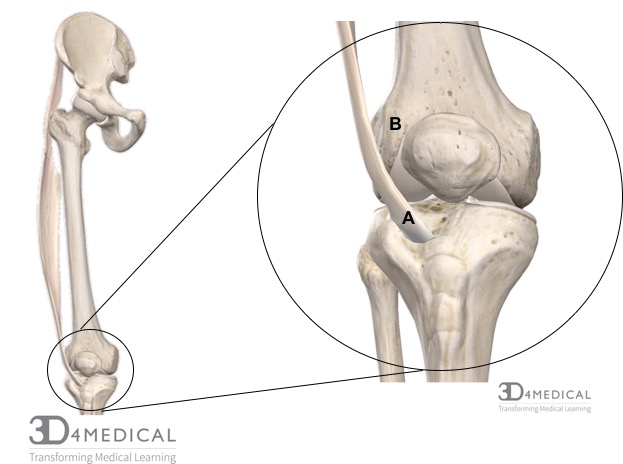
Iliotibial Band Friction Syndrome (ITBFS) is an injury that occurs over the lateral aspect of the knee. ITBFS occurs when the distal portion of iliotibial band (see figure A in the photo below) comes in contact and rubs against the lateral condyle of the femur (see figure B). To learn more about the iliotibial (IT) band see the muscular section of the pelvis.
Symptoms:
When friction between the IT band and the femoral condyle occurs, inflammation and even tendonitis can start causing pain and aching in the lateral side of the knee. When pain increases it is most likely to cause people to walk with a limp until the pain subsides.
Causes & Treatment:
Some of the most common causes of ITBFS are overtraining, running downhill or on uneven surfaces, and in some cases a direct trauma. For treatment, ITBFS can mostly be cured with physiotherapy that is focused on reducing the load on the IT band. Along with physiotherapy, other forms of treatment such as rest, anti-inflammatories, massage treatments, and stretching are also recommended.
Osgood-Schlatter Disease
Description:
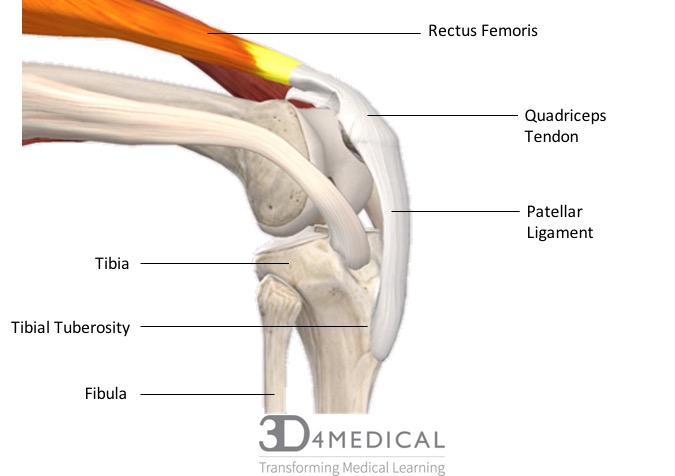
Osgood-Schlatter disease occurs when the quadriceps muscles pull on the patellar ligament which pulls and creates a stress on the tibial tuberosity during a growth spurt. During a growth spurt, the bones in children and adolescents possess an area of cartilage near the end of the bones called a growth plate that is designed for growth. The growth plate remains cartilage until the child has finished growing where it then hardens into a solid piece of bone. During this process, if there is excessive stress on the tibial tuberosity beyond normal levels it can cause pain and excessive bone growth on the tibial tuberosity. Osgood-Schlatter disease most commonly happens in children who are very physically active as there is an increased stress on the growth plate from sports that involve large amounts of running and jumping. That being said it is still possible for less active people to get Osgood-Schlatter disease.
Symptoms:
Symptoms may be experienced in both knees or in just one and are often initiated by running, jumping, and other strenuous physical activities. The stress that is created on the growth plate causing the excessive bone growth can be very painful and may cause a limp. In cases where both knees are affected, one may be more painful than the other.
Causes & Treatment:
The most common treatment for Osgood-Schlatter disease is rest from strenuous activity that increases the stress on the tibial tuberosity. Other additions to rest may be anti-inflammatory medications, as well as stretching routines that focus on taking some of the tension out of the quadriceps muscle group. In some cases, a short amount of rest might be needed and in other cases, it may be recommended that rest for several months may be needed for recovery.

Osteoarthritis
Description:
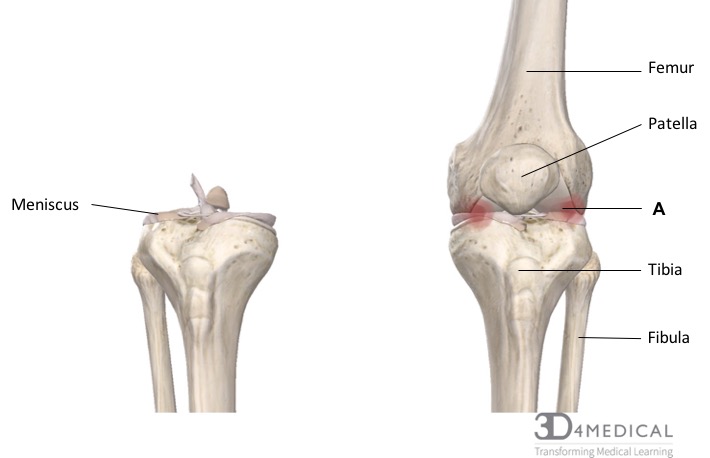
Osteoarthritis (os-tee-oh-ahr-thrahy-tis), also known as degenerative joint disease, occurs when cartilage covering the ends of bones breaks down, tears, or chips causing damage to the joint and pain (see photo below, figure A, for site of pain). It can affect any joint in the body but most commonly occurs in the knees, hips, lower back, neck, and small joints such as fingers and toes. In the knee, the meniscal cartilage provides a smooth, cushioned barrier that allows the articulating surfaces of the femur and tibia to glide past each other with ease. Osteoarthritis causes the meniscus to break down causing an inflammatory response and stiffness in the joint. In certain cases, the meniscus may deteriorate so significantly that the distal end of the femur and the proximal tibia can start to break down and can even develop growths called spurs. When the femur rubs against the tibia it can cause serious bone damage and intense pain. Osteoarthritis is most common in people over the age of 65 but can still occur in people of any age as risk factors such as obesity, previous joint injury, and weak muscles increases.
Symptoms:
The most common symptoms of osteoarthritis include pain, stiffness, and swelling. Stiffness is most commonly experienced first thing in the morning or after resting for long periods of time, and swelling is most likely to occur after prolonged activity. It is also common that a “grating” or “scraping” feeling is experienced when moving the knee. As the cartilage degenerates, symptoms start to increase in severity rather than appear suddenly.
Causes & Treatment:
There are various factors that can make people more predisposed to developing Osteoarthritis. These factors include both genetic and lifestyle traits. In terms of genetics and gene mutations, there are conditions that impair the body’s ability to produce collagen which is the protein that makes up cartilage. People who have this genetic trait can develop osteoarthritis as a teenager and may need a surgical procedure to provide relief. Other genetic mutations may cause abnormalities in bone growth between the femur and the tibia causing a defect in the way the bones fit together. This can result in increased friction in the joint and faster wear of the meniscal cartilage. When it comes to lifestyle, studies have found that increased weight and the stress it places on the joints causes the meniscal cartilage to break down at a faster rate. This is not only due to the extra weight on the joint but also due to the inflammatory chemicals known as cytokines that are stored in fat tissue.
In most cases, osteoarthritis can be managed by exercising. This includes strength building exercises to strengthen the muscles around the joint to take away some of the burden, range-of-motion exercises to help increase flexibility and decrease stiffness, as well as stretching activities to reduce stiffness and pain. In the cases that cannot be treated with exercise, other treatments such as pain and anti-inflammatory medications, assistive devices or orthotics, and joint repairing surgeries can be used.
THE FEMALE KNEE
Anterior Cruciate Ligament Injuries
Description:
Females are 4-10x more likely to tear their anterior cruciate ligament (ACL) than males. The ACL extends from the anterior intercondylar area of the tibia to the posterior part of the medial surface of the lateral condyle of the femur. It provides rotational stability to the knee and prevents anterior movement of the tibia off of the femur. Pinning down why females are at a greater risk to one specific reason is impossible, as many factors could play a role. There are several anatomical and physiological variables that predispose the female to a greater number of ACL injuries.
The first anatomical factor that plays a role is regarding the intercondylar notch. This notch is the area between the medial and lateral epicondyles of the femur and is where the ACL passes through. On average, the female notch is 17.4 mm compared to the male notch which is 19.3 mm. This difference of 1.9mm may not seem like much, but it is actually very significant. This smaller notch leads to a smaller ACL, which in turn leads to a weaker ACL. The ACL being weaker in females is one of the reasons we see more ACL injuries in female athletes.
The second anatomical factor is the greater Q angle seen in females. The Q angle is a measurement of pelvic width, and it construes the angle of which the femur is at when it connects to the knee joint. The average Q angle in females is 180°. This is 50° greater than the average male Q angle. This increased Q angle can predispose the knee to greater stress due to the torsion applied between the femur and tibia. The increased Q angle can also throw off alignment and biomechanics. It can contribute to joint laxity, as an increased Q angle is also related to increased flexibility. The Q angle plays a role in several mechanisms throughout the body, and each one of them can predispose the ACL to an increased injury rate.
The third anatomical factor, also the least talked about, is the hamstrings: quadriceps ratio (H:Q ratio). This ratio is measured by taking the strength of the hamstrings and dividing it by the strength of the quadriceps. Normal H:Q ratio scores range anywhere from 50% – 80%. Females tend to have a lower H:Q ratio than males, around 40% – 60% compared to males who clock in at 70% – 85%. The hamstrings and ACL are agonists to each other in knee stabilization, so if the hamstrings are weaker than the quadriceps, the ACL will have to compensate for the hamstrings and provide more stability to the knee. There will be more force applied to the ACL as the hamstrings are not providing adequate stability. This added force is one of the reasons females are more likely to experience ACL injuries.
The last factor is not anatomical, but instead physiological. Female sex hormones such as estrogen, progesterone, and relaxin are known to cause joint laxity. This laxity is caused by a reduction in fibroblast and collagen synthesis, which decreases structural framework in the body. There are estrogen and progesterone receptors on the ACL. During the ovulatory phase of a female’s menstrual cycle, estrogen levels surge. This increase of hormones means more hormones bind to the ACL directly. A higher percentage of ACL tears occur in the ovulatory phase of the menstrual cycle (days 10-14). Fewer injuries occur in the follicular phase (days 1-9) when hormone levels are lower.
Combine all of these factors discussed, and it is not hard to believe females are 4-10x more likely to tear their ACL than their male counterparts.
Diagnosis:
Often ACL tears can be diagnosed through a physical exam. During the exam, your doctor may move your knee into a variety of positions to assess the range of motion and overall function of the joint. The Lachman test is the most accurate test for detecting an ACL tear. The examiner will pull your tibia anteriorly and observe how much movement occurs. An intact ACL should prevent forward translational movement of the tibia on the femur. You may need other tests to rule out other causes and to determine the severity of the injury. These tests may include x-rays, MRI’s, and ultrasound.
Complications:
An ACL injury results in a significant risk of developing arthritis within 10 to 15 years. Around 70-80% of people that tear their ACL develop arthritis in that timeframe. This is particularly troublesome because most ACL injuries occur in young people, meaning that arthritis could set in at a very early age. The actual injury and the knee’s inflammatory response to the trauma seem to be the reasons behind this.
Treatment and Surgical Interventions:
If your ACL is torn completely, you will need surgery, especially if you are an athlete. If your ACL is not torn completely, treatments such as first aid, non-steroidal anti-inflammatory drugs, knee brace, and physical therapy may be sufficient in rehabbing it. Surgery combined with physical therapy can often rehab a torn ACL in 12 months.
Anterior and Posterior Ankle Impingement
Description:
Is defined as pain in the ankle due to an impingement in one of two areas: anterior and posterior. Pain is
caused by mechanical obstruction due to osteophytes (I.e., a bony outgrowth associated with the
degeneration of cartilage at joints) and/or entrapment of various soft tissue structures due to
inflammation, scarring or hypermobility.
Anterior impingement is often known as “athlete’s ankle” or “footballer’s ankle”, which is caused by
repeated dorsiflexion, microtrauma, and repeated inversion injury to structures such as the articular cartilage. Posterior impingement is often known as “dancer’s heel”, which is generally subtle in nature, occurring in athletes who routinely plantarflex, such as ballet dancers, jumping athletes, and those who kick. Posterior impingement is a common cause of chronic ankle pain. There are many causes to posterior impingement such as: bony or soft tissue impingement, specifically flexor hallucis longus irritation, inversion trauma/sprain, and forced plantarflexion causing anterior sheering (I.e., change of direction) of the tibia.
Symptoms:
Commons symptoms of anterior and posterior ankle impingement are pain, swelling, and limitation of
ankle dorsiflexion.
Treatments:
Conservative methods are recommended to be taken for at least the first 3 months, if no progress, then
surgery becomes an option. Current literature favors surgical intervention as a treatment
Physical Therapy
Treatment focus’ on increasing available joint space for more mobility and less pain from physical
activity. For acute symptoms, a period of rest and an avoidance of provocative activities are
recommended. For chronic cases, shoe modifications, including heel lift orthoses to prevent
dorsiflexion.
Surgery
Arthroscopy has been found to be a useful method to treat patient’s ankle impingements, also
debridement (I.e., the removal of damaged tissue or foreign objects from a wound), and flexor hallux
longus release.
Prevention:
To prevent posterior ankle impingements, protective ankle dorsiflexion taping is recommended.
Ankle Sprain

Figure 6. A visualization of an ankle sprain
Description:
An ankle sprain is where one or more of the ligaments of the ankle are partially or completely torn.
Ankle sprains are a common injury. Inversion-type lateral ligament sprains represent approximately 85%
of all ankle sprains and are most prevalent in sports populations. Most common risk factor is previous
history of ankle sprains.
Of the lateral ankle ligament complex the most frequently damaged one is the anterior talofibular
ligament (ATFL). On the medial side, the strong, deltoid ligament complex [posterior tibiotalar (PTTL),
tibiocalcaneal (TCL), tibionavicular (TNL) and anterior tibiotalar ligaments (ATTL)] is injured with forceful
pronation and rotation movements of the hindfoot. A syndesmosis (I.e., high ankle) sprain occurs with
combined external rotation of the leg and dorsiflexion of the ankle.
Symptoms:
Common symptoms include swelling, tenderness, bruising, and/or paraesthesia (I.e., an abnormal
sensation, typically tingling or pricking (“pins and needles”), caused mainly by pressure on or damage to
peripheral nerves).
Grading system:
Traditional Grading system
• Grade I represents a microscopic injury without stretching of the ligament on a macroscopic
level.
• Grade II has macroscopic stretching, but the ligament remains intact.
• Grade III is a complete rupture of the ligament.
3 Graded Classification System
• Grade I Mild – Little swelling and tenderness with little impact on function
• Grade II Moderate – Moderate swelling, pain, and impact on function. Reduced proprioception,
range of motion and instability
• Grade III Severe – Complete rupture, large swelling, high tenderness loss of function and marked
instability
Treatments:
Physical Therapy
Mild Ankle Sprain
Natural full recovery occurs within 14 days, followed with taping and follow ups to evaluate healing
progression.
Severe Ankle Sprain
1. Inflammatory (0-3 days)
Goals: Reduction of pain and swelling and improve circulation and partial foot support
Most common protocol is PRICE (Protection, rest, ice, compression, elevation)
• Protection: Protect the ankle from further injury by resting and avoiding activities that may
cause further injury and/or pain
• Rest: Advise rest for the first 24 hours after injury, possibly with crutches to offload the injured
ankle and altering work and sport and exercise requirements as needed
• Ice: Apply a cold application (15 to 20 minutes, one to three times per day)
• Compression: Apply a compression bandage to control swelling caused by the ankle sprain
• Elevation: Ideally elevate ankle above the level of the heart, but as a minimum, avoid positions
where the ankle is in a dependent position relative to the body
2. Proliferative (4-10 days)
Goals: Recovery of foot and ankle function and improved load carrying capacity.
Gradual increase in activity level, guided by symptoms. Practice foot and ankle functions like range of
motion, active stability and motor coordination. Tape/brace once the swelling has gone down.
3. Early Remodeling (11-21 days)
Goals: Improve muscle strength, active (functional) stability, foot/ankle motion, mobility (walking,
walking stairs, running)
Provide information about possible preventative measures and advice for proper shoes to wear during
sports activities, regarding sports type and surface. Have patient practice balance, muscle strength,
ankle/foot motion and mobility. Work on dynamic stability with use of different types of surfaces toincrease difficulty with improvement. Provide advice on taping and bracing during activities until the patient
can confidently perform static and dynamic balance and motor coordination exercises.
4. Late Maturation and Remodeling
Goals: Improve the regional load-carrying capacity, walking skills and improve the skills needed during
activities of daily living as well as work and sports.
Patient should practice and adjust foot abilities (functions and activities) by practicing motor
coordination skills while performing mobility exercises, continuing to progress the load-bearing capacity
as described above until the pre-injury load-carrying capacity is reached, increase the complexity of
motor coordination exercises in varied situations until the pre-injury level is reached and encourage the
patient to continue practicing at home.
Chronic Ankle Instability
Description:
Chronic ankle instability is a reoccurring injury of the ankle when lateral sprains (inversion sprains) consistently occur. It stretches out the ligaments in the ankle which makes it weaker therefore more susceptible to sprains.
Symptoms:
- Repeated occurrences of ankle sprains
- Persistent discomfort and swelling
- Pain and tenderness
- The ankle feeling wobbly or unstable
Causes:
Chronic ankle instability is caused by poor rehabilitation from ankle sprains. By not adequately doing rehabilitation, the ankle is remains weak and unstable. An unstable ankle is more likely to sprain again and the main cause of chronic ankle instability is re-occurring ankle sprains.
Treatment & Surgical Intervention:
Physiotherapy
Initial Treatment (with in the first 48-72 hours)
- RICE (Rest, ice, compression, and elevation)
- If possible, bear weight in the usual heel-toe pattern. Partial weight will do too. By bearing weight it will help reduce pain and swelling,
- Gentle soft tissue massage
Restore range of motion and balance
- Seated Balance Board Exercise
Restore Strength
Surgery
Surgery is dependent on a series of factors:
- Activity Levels
- Severity Levels
- Response to Exercises
If there is a lack of response to physiotherapy exercises and nonsurgical approaches and there is a high level of activity then surgery is a viable option.
The surgery will vary from individuals as the injured ligaments and severity will vary from individuals.
