Lower Limb
Joints, Ligaments and Connective Tissues
The Knee Joint
The knee is the most weight-bearing joint in the human body, transferring weight from the femur to the tibia. The joint is a synovial hinge joint formed between the femur, tibia, and patella. As a hinge joint, the knee permits flexion, extension, and very limited rotation. Each articulating surface forming the knee joint is covered in a thin layer of hyaline cartilage; creating a smooth surface to facilitate tissues to glide over each other in movement. The joint capsule which surrounds the bones of the knee is made of fibrous connective tissue which provides the joint with strength and lubrication. Lining the joint capsule is a synovial membrane that fills the space in-between bony structures to lubricate the joint and reduce friction between articulating surfaces. Numerous connecting ligaments are used to improve stability, strength, and to hold the joint in place.

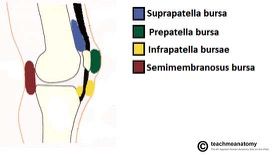
Along with synovial fluid within the joint, there are small pockets of fluid called bursae which reduce friction from the movement of tendons in the joint. The four main bursae found within the knee joint include the suprapatellar bursa, prepatellar bursa, infrapatellar bursae, and the semimembranosus bursa. The suprapatellar bursa is important for reducing friction between the bony structures of the patella and femur.
Along with bursae, there are other forms of cushions known as articular fat pads which protect the knee from external stress. The largest articular fat pad is the infrapatellar fat pad which cushions the patellar ligament during flexion/extension of the knee by absorbing shock. The articular fat pads, as well as the bursae contained in the joint capsule, are the main structures responsible for the protection and lubrication of the knee.
Knee Ligaments
Patellar ligament
The patellar ligament is a thin flat band of connective tissue around 2 to 3 inches long connecting the distal end of the patella to the tibial tuberosity. It is a continuation of the quadriceps femoris tendon which connects the quadriceps group to the patella. At birth, the patellar ligament doesn’t exist. It isn’t until a mass of cartilage within the quadriceps tendon ossifies to form the patella, it then divides the quadriceps tendon into two distinct parts. Once the distal portion of the quadriceps tendon is connected to the patella and tibia it is then called the patellar ligament. Functionally, the patellar ligament has an important role in the extension of the thigh. When the muscles of the quadriceps femoris group contract, it pulls on the patella via the quadriceps tendon; the patella is pulled proximally; the patellar ligament then pulls on the tibia to extend the leg at the knee. This action is important for walking, running, jumping, and kicking.
Oblique popliteal ligament
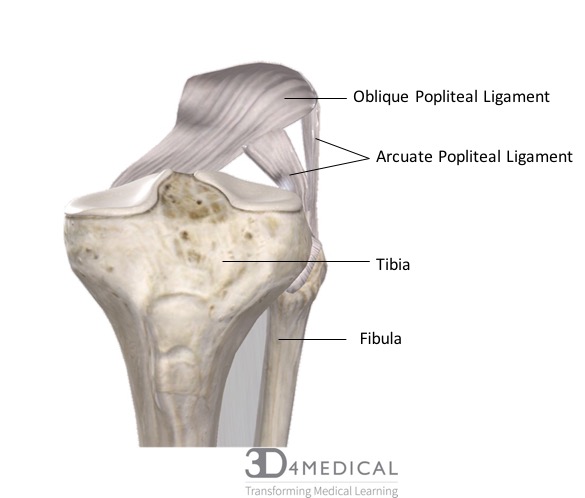
The oblique popliteal ligament is a broad, flat band of connective tissue that crosses the back of the knee. It originates on the medial condyle of the tibia as an extension of the semimembranosus muscle’s tendon and inserts on the lateral condyle of the femur. The ligament provides important reinforcing properties along with the arcuate popliteal ligament to the posterior aspect of the knee.
Arcuate popliteal ligament
The arcuate popliteal ligament is a broadband in the shape of a “V” that supports the posterior aspect of the knee. It originates on the head of the fibula and inserts on both the intercondylar area of the tibia and the lateral epicondyle of the femur. Just like the oblique popliteal ligament the arcuate popliteal ligament also helps to reinforce the posterior aspect of the knee.
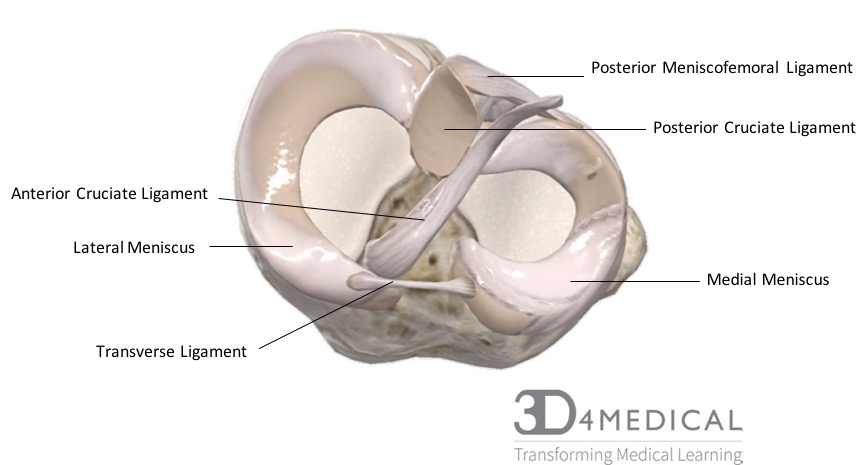
Anterior cruciate ligament (ACL)
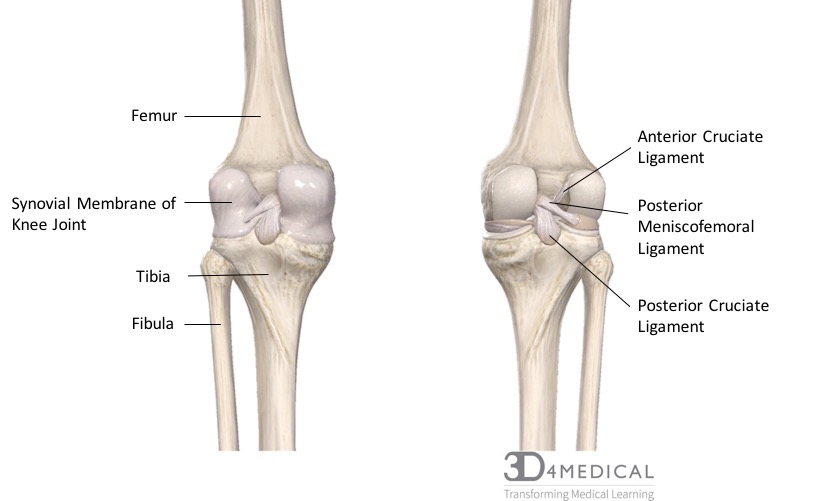
The anterior cruciate ligament (ACL) is a small thin ligament connecting the anterior intercondylar area of the tibia to the posterior part of the medial surface of the lateral condyle of the femur. In terms of movement of the knee, the ACL resists anterior displacement of the tibia. Spraining or tearing of your ACL is one of the most common knee injuries. Both the anterior cruciate ligament and the posterior cruciate are found within the knee joint and cross each other to form an “X”.
Posterior cruciate ligament
The posterior cruciate ligament (PCL) is the pairing ligament within the knee joint that forms an “X” with the anterior cruciate ligament. The PCL connects the posterior intercondylar area of the tibia to the anterior part of the lateral surface of the medial condyle of the femur. In terms of movement of the knee, the PCL resists posterior displacement of the tibia. Together the PCL and ACL work to control forward and backward motion of the knee.
Helpful Hint
To remember the position and direction of the ACL and PCL ligament, cross your fingers where your middle finger crosses over your index finger to mimic an ‘X’. The middle finger mimics the ACL running lateral-medial, originating anterior and inserting posteriorly; while the index finger mimics the PCL running medially to laterally, originating posterior and inserting anteriorly.
Tibial collateral ligament (MCL)
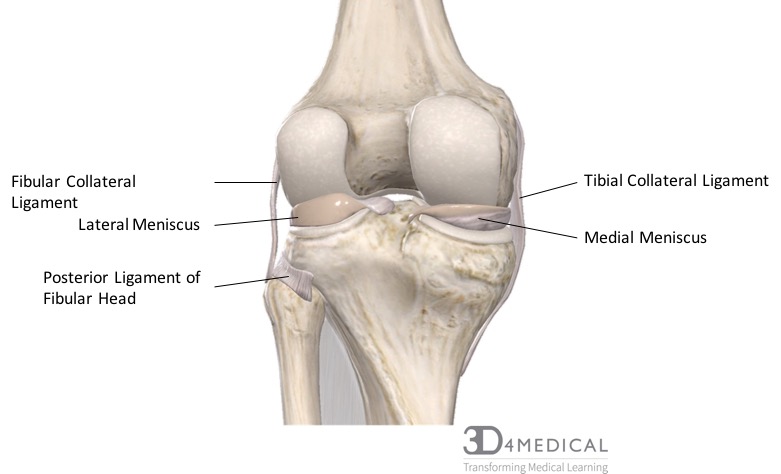
The tibial collateral ligament, also called the medial collateral ligament, is one of the four main ligaments of the knee joint along with the ACL, PCL, and LCL. It runs along the medial side of the knee from the femur’s medial epicondyle to the medial margin and surface of the tibia. The ligament can be found under the insertion points of gracillis, sartorius, and semitendinosus. Functionally the MCL keeps the knee stable through its full range of motion as well as preventing lateral movement from lateral/valgus forces. Compared to the fibular collateral ligament or LCL the MCL is a lot less flexible, therefore making it more prone to injury.
Fibular collateral ligament (LCL)
The fibular collateral ligament also called the lateral collateral ligament (LCL), is a cord-like ligament that runs along the lateral side of the knee. It originates on the lateral epicondyle of the femur and inserts on the head of the fibula. Similar to the MCL the LCL is also responsible for stabilization of the knee and prevents medial movement of the tibia from medial/varus forces.
Medial/lateral menisci
In the space between the femur and the tibia are two C-shaped discs of tough, rubbery fibrocartilage known as the medial and lateral menisci (plural for meniscus). The purpose of the meniscus is to act as shock absorbers between the leg bones during strenuous activity. Each meniscus fits in the shallow depression in the tibial plateau and in the event of injury, will prevent the knee from working right. The most common ways of injuring the menisci are from sudden twisting or turning while the foot is planted, and the knee is bent.
Medial/ Lateral patellar retinaculum
The medial patellar retinaculum is an aponeurosis, which is facia connecting muscle to the bone that resembles a tendon of the vastus medialis muscle. It travels around the patella medially and attaches to the medial condyle of the tibia. Both the medial and lateral patellar retinaculum play a big role in forming the fibrous capsule around the knee. The lateral patellar retinaculum is very similar to the medial with the exception that it is an aponeurosis of the vastus lateralis muscle and travels around the patella just laterally. The patellar retinaculum aids in the extension of the knee and is vital in running, walking, and kicking.

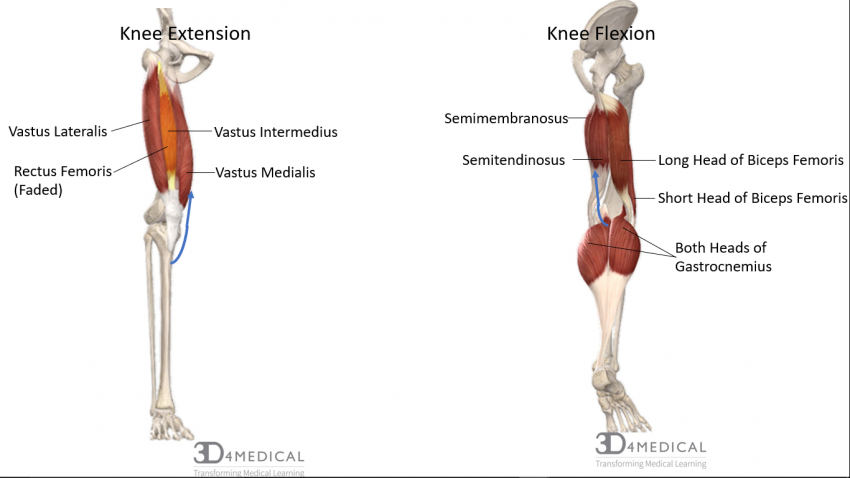
Figure 6. Diagram demonstrating the muscles activated during knee extension and knee flexion.
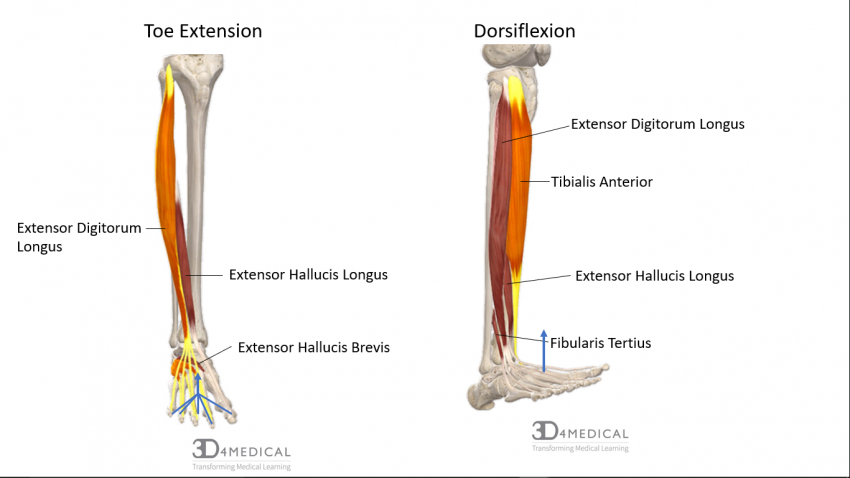
Figure 7. Diagram demonstrating the muscles activated during toe extension and dorsiflexion.
As is the case with wrist flexion and extension, the dorsi-flexors and plantar-flexors of the foot can move the foot or toes on their own, or both at the same time during a full contraction.
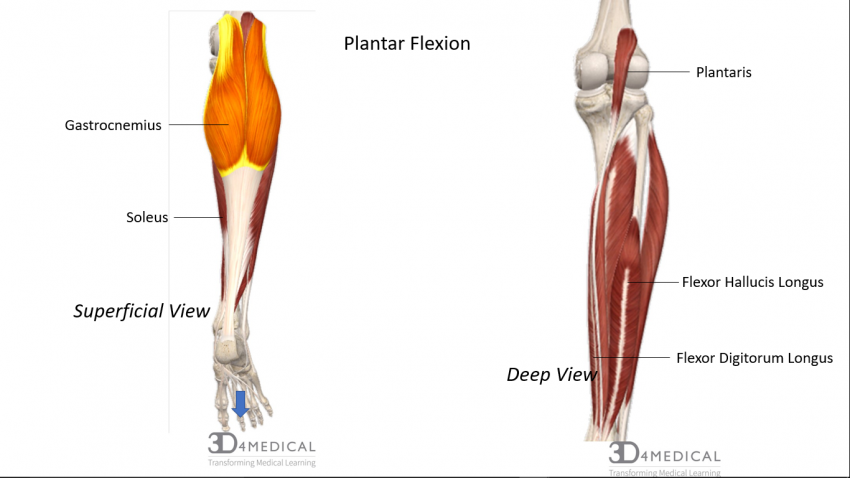
Figure 8. Diagram demonstrating the posterior view of the muscles activated during plantar flexion.
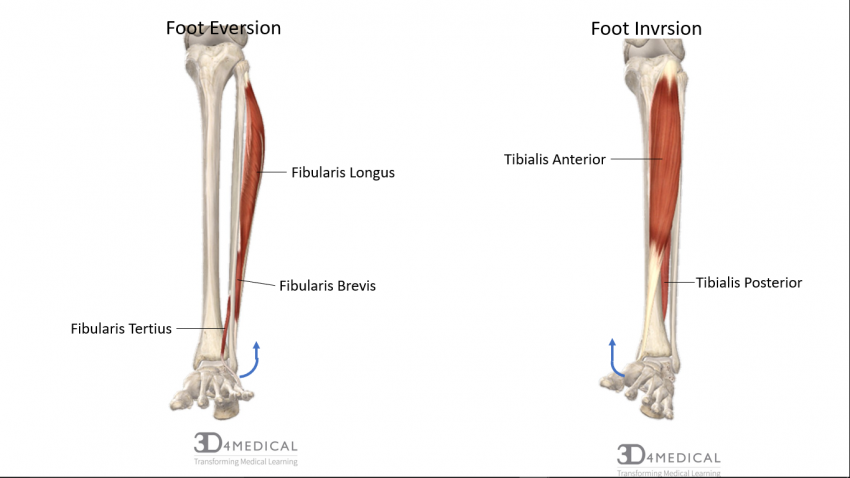
Figure 9. Diagram demonstrating the anterior view of the muscles activated during ankle inversion and eversion.
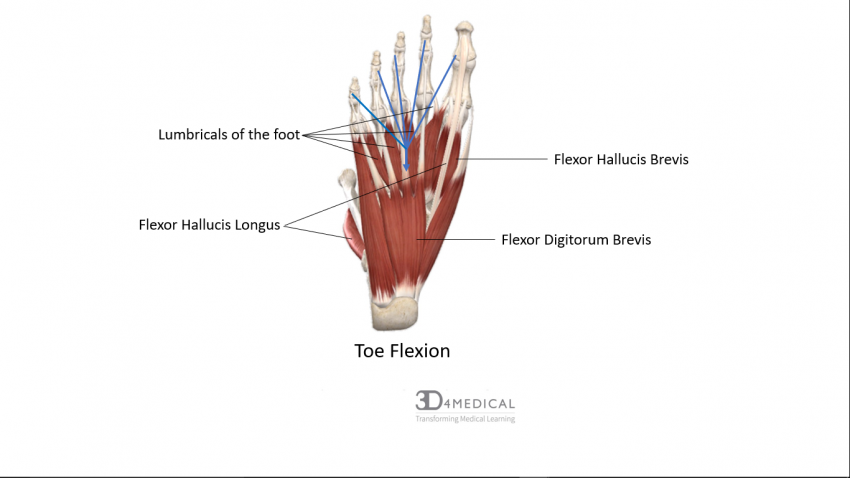 Figure 10. Diagram demonstrating the muscles activated during toe flexion.
Figure 10. Diagram demonstrating the muscles activated during toe flexion.
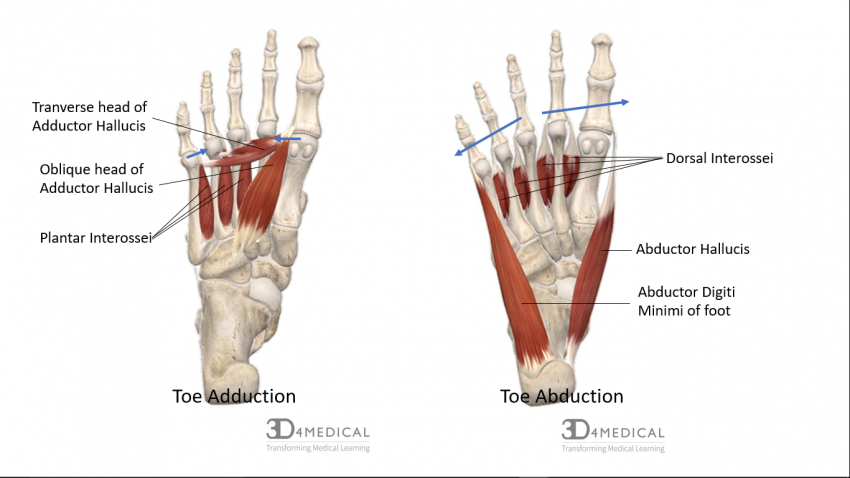
Figure 11. Diagram demonstrating the muscles activated during toe adduction and abduction.
The Ankle Joint
The ankle is a synovial joint, which contains a joint cavity that is fluid-filled where articulating bones contact each other. The joint is classified as a uniaxial because its only actions include bending and straightening motions along one axis.
Ligaments
The ligaments of the ankle play a major role in stabilization, control, and protection of the joint. The ligaments of the ankle are separated into the medial and lateral groups. The lateral group includes the anterior talofibular ligament (ATFL), posterior talofibular ligament (PTFL), and the calcaneofibular ligament (CFL). The medial group includes deltoid ligament, including the anterior tibiotalar ligament (ATTL), posterior tibiotalar ligament (PTTL), tibionavicular ligament (TNL) and tibiocalcaneal ligament TCL)]. Each ligament is connected to a mechanism of injury.
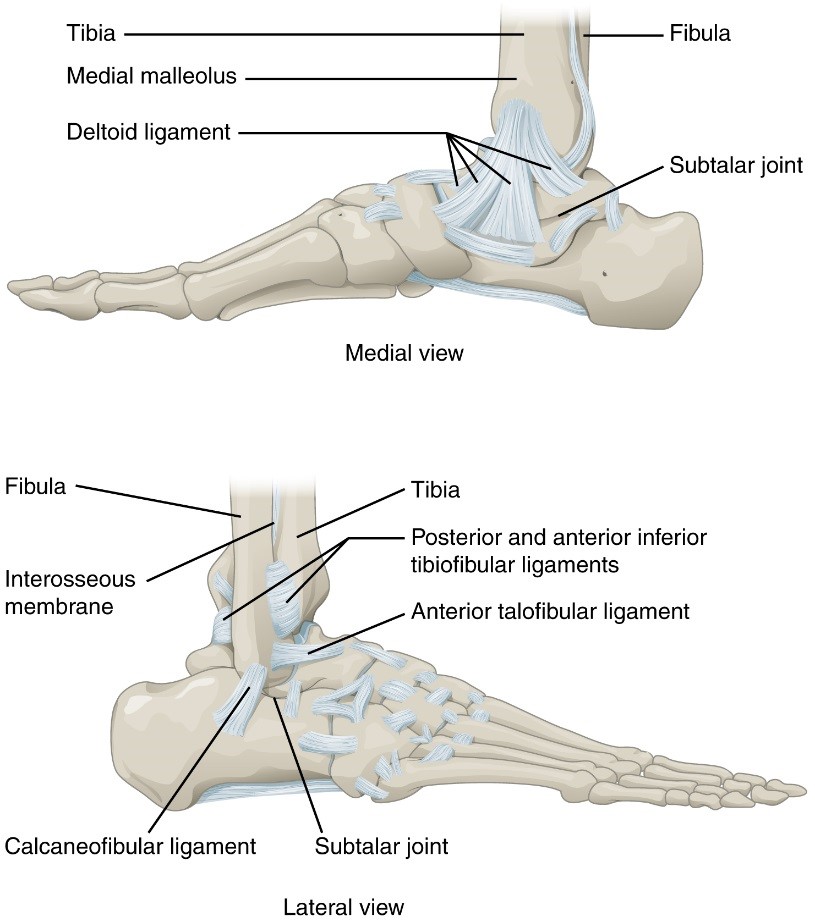
Figure 12. Diagramd demonstrating the medial (top) and lateral (bottom) views of the ankle ligaments.
| Lateral Ankle Ligaments | ||||
| Ligament | Proximal attachment | Distal attachment | Role | Mechanism of injury |
| Anterior Talofibular Ligament | Lateral Malleolus | Neck of Talus | Restrain anterior displacement of the talus.
Resists Inversion in plantarflexion. |
Inversion and plantarflexion
|
| Posterior Talofibular Ligament | Malleolar Fossa of Fibula | Lateral Tubercle of Talus | Resists posterior displacement of the talus. | Inversion and plantarflexion
|
| Calcaneofibular Ligament | Tip of Lateral Malleolus | Lateral Surface of Calcaneus | Aids Talofibular stability during Dorsiflexion.
Restrain inversion of the calcaneus. Prevent Talar tilt into Inversion |
Inversion and plantarflexion |
| Medial Ankle Ligaments | ||||
| Ligament | Proximal attachment | Distal attachment | Role | Mechanism of injury |
| Anterior Tibiotalar
Ligament |
Medial Malleolus | Head of Talus | Reinforces Ankle Joint.
Control Plantarflexion & Eversion |
Eversion |
| Posterior Tibiotalar
Ligament |
Medial Malleolus | Posterior Talus | Control Dorsiflexion | Eversion |
| Tibionavicular
Ligament |
Medial Malleolus | Dorsomedial Aspect of Navicular | Reinforces Ankle Joint | Eversion |
| Tibiocalcaneal
Ligament |
Medial Malleolus | Sustentaculum Tali of the calcaneus (acts like a shelf-like support of the talus) | Reinforces Ankle Joint | Eversion |
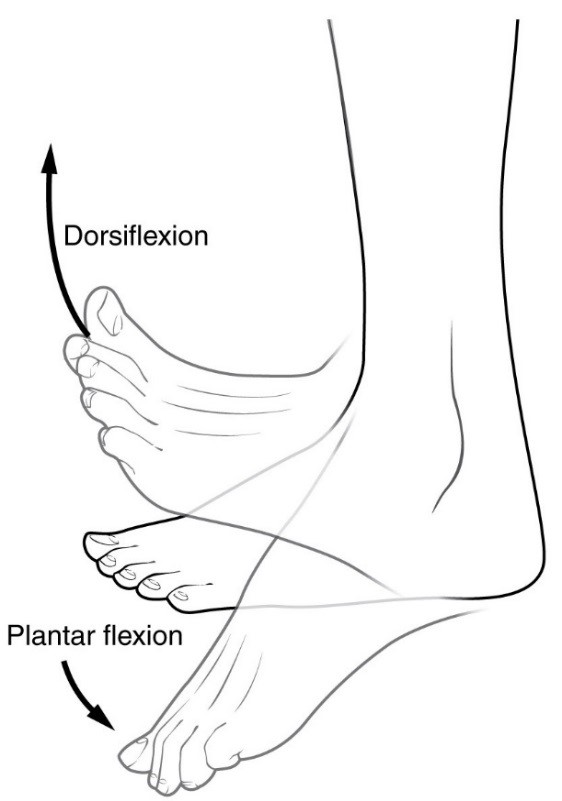

Figure 13. Diagram summarizing plantar flexion, dorsiflexion (left) and inversion and eversion (right) of the ankle.
