The Head and Neck
Clinical Conditions
CLINICAL CONDITIONS OF THE MUSCULOSKELETAL SYSTEM
Fontanelles
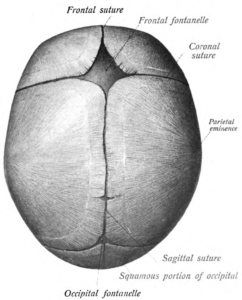
Figure 1. A visual representation of the fontanelles of the human skull from a superior perspective.
Description:
Fontanelles are gaps usually found on infants. These gaps are made up of soft membranous sutures between the cranial bones. There are six fontanelles found in the newborn’s skull. One on the anterior region of the skull, one on the posterior region of the skull, two mastoid fontanelles and two sphenoid fontanelles.
Symptoms:
- Misshapen skull
- Abnormal feeling
- Soft spots on a newborn’s head
Causes:
The fontanelles allow room for the head to pass through the birthing canal while still allowing for cranial growth post birth.
Treatment & Surgical Intervention:
The fontanelles should harden and close by the time the infant is 2 – 18 months old on its own. Each closure of the fontanelle varies depending on the location.
Cervical Lordosis
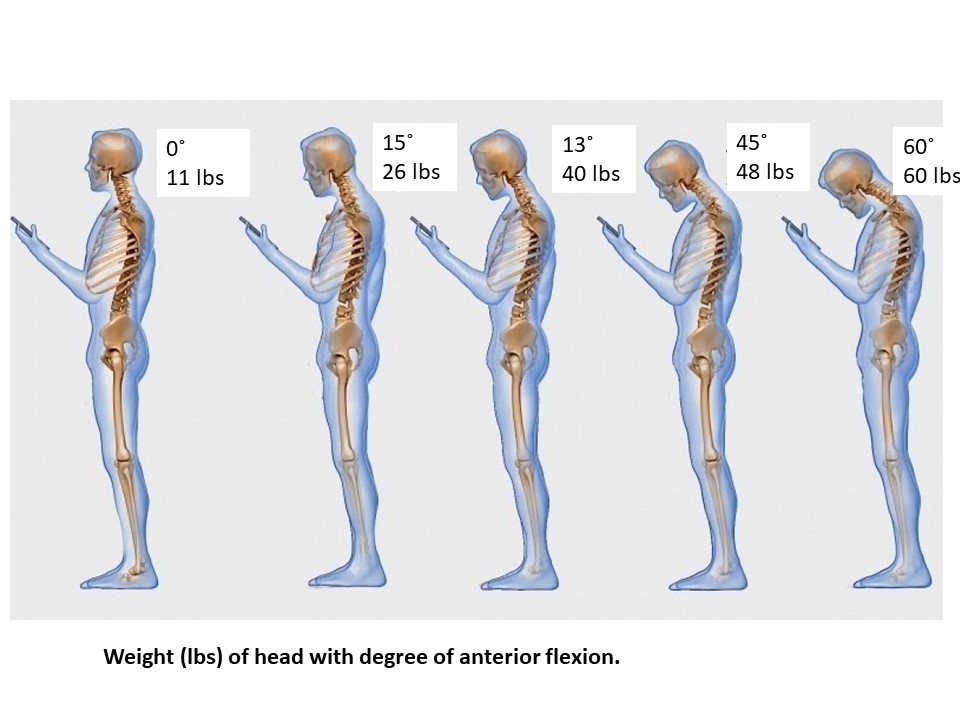
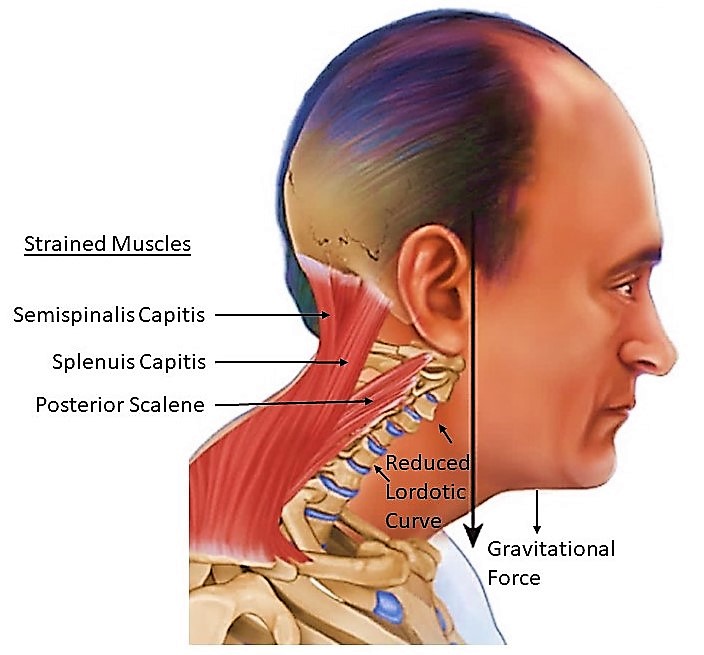
Figure 2. A visual representation of the cervical spinal curvature in an individual inflicted with cervical lordosis.
Description:
When the neck is constantly held in a flexed, anterior position, the posterior extensor muscles of the neck hold the neck up. For every inch the head protrudes forward and every ~10 degrees that the head tilts downward, the head adds ten pounds of added pressure on the neck. This pressure straightens the neck and causes muscular stress as well as reduces the curved positioning of the vertebrae and the neck is affected by gravitational forces on the head. Lordotic changes can be skeletal or muscular in nature.
Symptoms:
- Pain in neck
- Headaches
- Chronic tightness of the trapezius, levator scapula, splenius capitis, spleniuscervicis and semispinalis capitis.
Causes:
Decrease in lordotic curve often occurs when the head is repeatedly held in a forward position anterior to the trunk; looking down at a hand-held device or pushed forward at a computer, TV or driving.
Treatment:
Chiropractic intervention will help get the cervical vertebrae restored to the normal curve. Chiropractors will often send you home with some exercises to do on your own.
At home exercises:
- Neck Flexion
- Slowly tilt your head downwards to look at the floor then slowly bring it back to normal position
- Neck extension
- Slowly tilt your head upwards to look at the ceiling then slowly bring it back to normal position
- Cervical flexion/extension
- Put a towel behind your neck and hold it down the perform both the previous neck extension and nec
k flexion exercises. The towel will help restore the curve in your cervical vertebrae.
- Put a towel behind your neck and hold it down the perform both the previous neck extension and nec
- Neck Retraction
- Slowly draw your head back with your chin slightly angled downward then return back to normal. Look ahead the entire time.
- Upper neck nodding
- Lie on your back looking at the ceiling with a pillow behind your head. Super slowly bring your chin down to your chest. Be super careful when doing this as these muscles are often very tight.
Here is a video to demonstrate how to perform a couple of the exercises above:
Upper Crossed Syndrome
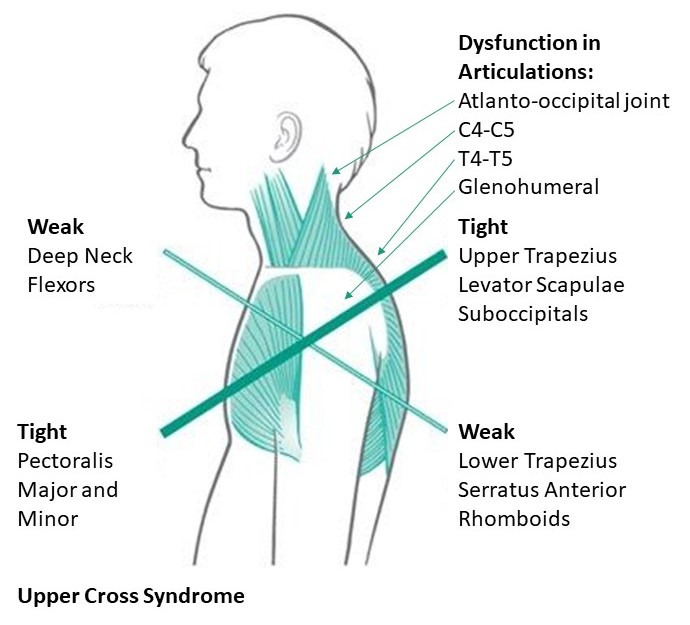
Figure 3. A visual representation of the anatomical characteristics commonly exhibited in an individual with upper crossed syndrome.
Definition:
Upper Crossed Syndrome is when the muscles of the neck and shoulders (often upper region of trapezius, and levator scapula) become extremely overactive and strained while the muscles in the front of the chest (often pectoralis major and minor) become shortened and tight. This means that the surrounding muscles become weak. Therefore, the front of the neck (cervical flexor muscles) and the lower shoulders (lower trapezius and rhomboid major and minor). The imbalance of upper crossed syndrome causes impaired function of joints of the neck and shoulder. Clinically of note is dysfunction in articulations: atlanto-occipital, between C4 and C5, T4 and T5, and decreased stability in the glenohumeral (shoulder) joints because of chronic rounded shoulder positioning.
Symptoms:
- Stiffness in the neck and or back
- Aches in the neck and or back
- Restricted range of motion in the neck or shoulders
Causes:
Sitting in a hunched over position, like sitting at a computer or sitting at a desk for a long period of time is the main cause of upper crossed syndrome. Another cause is the forward head posture. This often happens when people use cellphones, read books and drive.
Prevention:
Avoid activities that require having the head forward and shoulders rounded forward for long extended periods of times.
- Limit time using computers, cell phones, watching TV, or driving
- Take 15-20 minute breaks when staying in the hunched over position.
- Do cardiovascular activities for at least 30 minutes a day
- Stretch target weakened muscles
Treatment & Surgical Intervention:
Relaxation of overactive muscles and strengthening of under-active muscles exercises are the main course of treatment. A few suggestions from physical therapy professionals may be similar to the following:
- Lying down in neutral position to relax muscles
- Rotation of the shoulders back and down to engage lower trapezius and rhomboid muscles and improve shoulder positioning
- Also included are likely to be exercises for craniocervical flexion and relaxation of suboccipitals to decrease headaches.
Below is a link discussing exercises for Upper-Cross Syndrome and a link to a video showing one way to relieve tension and chronic pain of the trapezius. (Please consult a professional before undertaking exercises):
https://www.youtube.com/watch?v=ABEA0dcjsUc
Whiplash
Definition:
Whiplash is defined as trauma that occurs with sudden acceleration or deceleration of the head and neck relative to other parts of the body, typically during vehicle collisions or other mishaps (GDC, 2010). During whiplash, the muscles spasm in order to protect the spine, especially when there is instability of ligaments, contributing to the soft tissue damage with this type of trauma. Compression and stretching can cause deep tissue damage to the cervical facet capsular ligaments. The nuchal ligament may also tear causing instability.
Branches of nerves from the cervical dorsal rami track through capsular tissue and are susceptible to damage during whiplash. Nociceptors (sensory neurons that signal the brain of possible threat and are perceived as pain) are activated with muscle, ligament and subsequent joint capsule strain. The structural loading and mechanical failures experienced during whiplash can cause damage to the nerve anatomical structure leading to chronic pain. Neuropathic pain, inflammatory pain, nociceptive, pain and dysfunctional pain may be experienced.
Along with damage to the capsular ligaments within the facet joints, bruising of the menisci are likely to occur. Less likely, (not commonly observed) but possible, are fractures to the bony elements within the cervical region that are thought to be caused by severe loading.
This video offers an overview of the mechanics of whiplash injury. https://www.youtube.com/watch?v=U9CnRFj3rWE
Symptoms:
Symptoms are often referred to as WAD – whiplash associated disorders.
- Neck pain, stiffness, and/or tenderness
- Decreased cervical range of motion
- Point tenderness
- Headaches dizziness, numbness, sleep difficulties, fatigue,
- Neurological complaints
Causes:
The main cause of whiplash is when there is a rapid movement backward and then forward. There are two components, component one is the acceleration of the torso relative to the still-stationary head and neck, causes the first load displacement with neck hyper-extension. Depending on the direction of force and the availability of a head support to break the backward motion, such as a correctly positioned head-rest in a motor vehicle, the impact of this stage of whiplash may be significant. The second component is a fast, forward load displacement of the head and neck recoiling from the backward motion with hyper-flexion of the neck. Actions that can cause whiplash are:
- Car accidents
- Physical abuse (punched or shaken)
- Contact sports (football and martial arts)
- Horseback riding
- Cycling accidents
- Falls and blows to the head.
Treatment & Surgical Intervention:
Physiotherapist will often do a multimodal patient-centered approach to treatment appears to be most effective, especially when paired with collaboration on a treatment plan with the injured party, education, exercises, information on self-management including active coping strategies, self-efficacy and periodic assessment.
Wry Neck

Figure 4. A visual representation of an infant that is displaying symptoms of wry neck due to stiffness developed in facet joints between adjacent cervical vertebrae.
Definition:
Wry neck is the common name for spasmodic torticollis or cervical dystonia. It is a condition where the muscles of the neck are locking into a sustained involuntary contraction. These contractions are often presented in a twisting motion, repetitive movements (muscle spasms), or abnormal posturing of the neck (Crowner, 2007).
Symptoms:
- Rotation of the head or chin towards the shoulder
- Neck pain and stiffness
- Headaches
- Loss of movement
- Muscle spasms in the neck
Causes:
Wry neck is usually a neurological disorder. However, a neck trauma can also cause wry neck. A locked facet joint or a cervical disc injury are the main problems that arise from a neck trauma. This means that when the facet joint gets locked the nerve endings that are located in that joint get irritated, this is how the pain occurs.
Treatment & Surgical Intervention:
Gentle physical therapy can help to relieve pain and drug treatment such as Botox (botulinum toxin) has been shown to provide some pain management (Kongsaengdao et al, 2017). Surgical methods such as selective denervation and deep brain stimulation are in the early stages of development for treatment.
CLINICAL CONDITIONS OF THE RESPIRATORY SYSTEM
Allergic Rhinitis
Description:
Allergic rhinitis is a particular condition that is characterized by the onset of an inflammatory response inside the mucous membrane of the nasal cavity in response to exposure to a number of environmental agents, such as allergens, bacteria, and viruses. This inflammatory response can lead to a reduction in the diameter of the nasal pathways, which can impede upon gas exchange and drainage of fluid in these pathways.
Symptoms:
- Runny nose and nasal congestion
- Allergic conjunctivitis (irritation and redness of the eyes)
- Allergic shiners (formation of blue circles under the inferior eye lid)
- Coughing, sneezing, and irritation of the nose and mouth
- Bodily fatigue and weakness
- Bronchial hyperresponsiveness (excessive bronchial narrowing in response to inhalation of certain stimuli. This symptom is a strong predictor of asthma)
Mechanism & Diagnosis:
Similar to most cavities of the body, the nasal cavity is lined with a mucous membrane that consists of a few layers of specialized epithelial cells that are bound to a loose layer of connective tissue. When referring to the histology of the nasal cavity, it is initially lined with a short segment of stratified squamous epithelium, and a longer segment of pseudostratified columnar ciliated epithelium that extends throughout the respiratory tract and olfactory region. This lining is composed of predominantly columnar cells, but also contains ciliated, goblet, and basal cells. Collectively, these cells and surrounding bony structures are responsible for: increasing the surface area of the lining to help retain an adequate degree of moisture in the epithelium, creating turbulence in oncoming airflow to maximize filtration between the air and mucous lining, collecting sensory information throughout the walls of the tract, promoting cell adhesion, and producing and secreting a thin layer of mucus to help protect and preserve the structural integrity of the tract.
Under certain conditions, this delicate mucous membrane can become irritated and inflamed due to exposure to a number of environmental agents. This condition is referred to as rhinitis. A visual representation of the inflammatory response that develops in the nasal mucosa during rhinitis is provided in Figure 5. The most common agents that have shown to mediate an inflammatory response in the mucous membrane include: viruses, such as the rhinovirus, bacteria, such as streptococcal bacteria, and allergens, such as pollens, dust, and molds. According to the research, rhinitis can be subdivided into several different categories based on the suspected etiology. Some of these categories include: allergic, idiopathic perennial non-allergenic, infectious, hormonal, medication-related, atrophic, and systemic disease-related. But among all these categories, allergen-mediated rhinitis (or “hay fever”) has shown to be the most prevalent in society, affecting “60 million people worldwide [yearly]…[and yielding] a prevalence of 10-30% in adults and 40% in children” (Min, 2010, p. 65). Upon exposure to various allergens, individuals with sensitized immune systems will produce immunoglobin (IgE), more commonly referred to as antibodies, which will activate mast cells, stimulating the release of a number of inflammatory-inducing molecules. Some of these molecules include: histamine, heparin, leukotrienes, and cytokines. The histamine that is released will mediate an excess release of mucus from the goblet cells of the mucous membrane, and will often initiate an irritation response. The leukotrienes and cytokines that are released will recruit and activate eosinophils, which are a common type of white blood cell that are responsible for combating pathogens. The migration of the eosinophils to the region of irritation will stimulate an inflammatory response, which will reduce the diameter of the respiratory pathways. In conjunction with the build-up of excess mucus, this will provide a congested sensation in the nasal pathways.
When referring to the diagnostic process, evaluating the patient’s current symptoms and undergoing a number of diagnostic tests are common procedures when attempting to detect allergic rhinitis. One of the most common diagnostic tests that are administered when testing for allergic rhinitis is skin tests. Some skin tests include: scratch, prick/puncture, intradermal, and patch tests. The main premise behind these tests is that if an individual is sensitive to a specific allergen, the affected area of skin should experience a hypersensitive response when exposed to this allergen. Although this testing modality has shown to merit a certain degree of validity and reliability, a reaction exhibited by the skin isn’t always representative of what would occur in the nasal cavity, as certain drugs, such as antihistamines, diseases, such as dermatologic disease, and the testing environment can skew the results. Another approach to diagnosing allergic rhinitis is through measuring one’s serum specific IgE levels via a radioallergosorbent test (RAST), multiple allergen simultaneous test (MAST), and the capsular hydrophilic carrier polymer system (CAP). Although RAST has shown to be effective at detecting IgE levels, this modality requires a radioactive isotope, expensive equipment, and cannot detect multiple antibodies simultaneously. Alternatively, MAST utilizes a photo reagent instead of a radioactive isotope, is rather inexpensive and ubiquitous, and possesses the ability to detect multiple antibodies during a given application. In addition to this, MAST is less invasive and isn’t impacted by a number of extraneous variables, such as antihistamines and dermatologic disease. CAP, which is an in vitro approach that focuses on collecting blood samples via a pin prick test and monitoring allergen dynamics in the blood plasma when exposed to a long chain of cellulose polymers. Since antigens have a high degree of affinity to the cellulose polymer compound utilized in this procedure, CAP is able to accurately detect changes in IgE levels in response to a variety of different allergens.
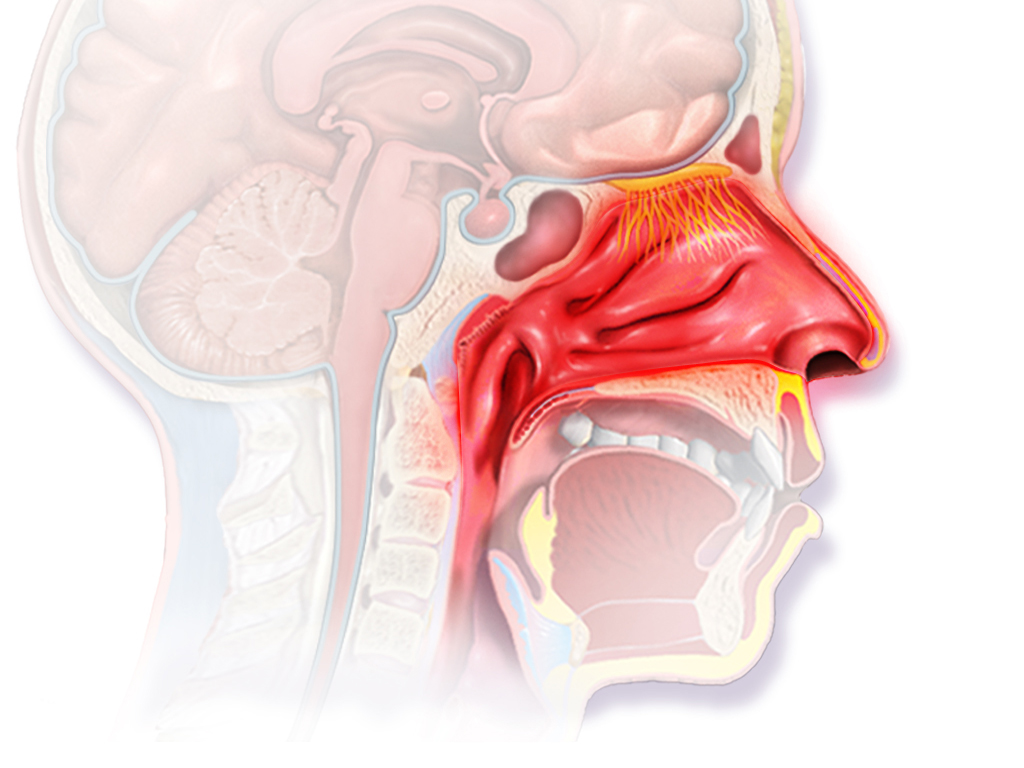
Figure 5. A visual representation of the inflammatory response that occurs in the mucous membrane lining of the nasal cavity during allergic rhinitis. (Image retrieved from: https://commons.wikimedia.org/w/index.php?search=allergic+rhinitis&title=Special%3ASearch&profile=default&fulltext=1#/media/File:Blausen_0015_AllergicRhinitis.png).
Treatment & Surgical Intervention:
Approaches that can be used when aiming to treat allergic rhinitis include: avoiding exposure to allergens that mediate a hypersensitive response in the body, pharmacological treatment, and immunotherapy. The pharmacological approach to treating allergic rhinitis is usually formulated based on the severity and duration of the symptoms exhibited by the patient. In general, oral and intranasal antihistamines, intranasal corticosteroids, leukotriene receptor antagonists (LTRAs), and anti-IgE antibodies are commonly used when treating allergic rhinitis. If the patient experiences prolonged symptoms while taking any of these medications, they are then instructed by the practitioner to revisit for a check up after 2-4 weeks under AR guidelines. Immunotherapy operates on the premise of gradually, incrementally, and systematically injecting allergen extracts into the body subcutaneously to mediate a hypersensitive response. Over an extended period of time (i.e., years of treatment), IgE levels in the blood plasma will begin to decrease, and IgG4 levels will begin to rise, resulting in a desensitization of the immunological mechanism of the body when exposed to previous hypersensitivity-inducing allergens. According to the research, this treatment approach has shown to improve bodily tolerance to specific allergens through facilitating an increase in the various chemical pathways associated with suppressing a hypersensitive response, such as T regulatory cells cytokines, TGF beta, and IL 10.
Sinusitis
Description:
Sinusitis is a particular condition that is characterized by the onset of an inflammatory response in the paranasal sinuses as a result of exposure to a number of pathogenic and allergenic agents, such as bacteria, viruses, and pollen. This local inflammation can play a role in reducing the diameter of the passageways that connect the paranasal sinuses to the nasal cavity, which can often lead to an over-accumulation of fluid and build-up of pressure in the paranasal sinuses.
Symptoms:
It is important to note that there are multiple classifications of sinusitis. Acute sinusitis occurs when the infection lasts for up to four weeks. Recurrent acute sinusitis occurs when an individual experiences four or more reoccurring bouts of sinusitis within a given calendar year. Subacute sinusitis occurs when symptoms last between four to twelve weeks, which marks the transitional period where acute sinusitis may manifest into a chronic condition. Chronic sinusitis occurs when the condition lasts for twelve or more weeks with a minimum of two primary symptoms exhibited. Acute exacerbation of chronic sinusitis occurs when symptoms exhibited in chronic sinusitis begin to exacerbate, then return to original levels when treated.
Generally, sinusitis is divided into acute and chronic categories. Some of the primary symptoms associated with sinusitis include:
- Postnasal drainage (drainage of thick, discoloured excess mucus secretions down the throat)
- Obstruction of nasal pathways (congestion)
- Inflammation deep to the skin around the eyes, checks, and forehead
- Reduced sense of taste and smell among adults, and frequent coughing in children
Some of the other symptoms include:
- Aching pain of the upper jaw, teeth, and ears
- Frequent coughing
- Sore throat
- Nausea
- Fatigue and weakness
- Halitosis (chronic bad breath)
Mechanism & Diagnosis:
Surrounding the nasal cavity, there are a number of specialized hollow cavities. These cavities, which are commonly referred to as the paranasal sinuses, are a collection of four air-filled chambers that form in the frontal, maxillary, sphenoid, and ethmoid bones of the skull. Similar to the nasal cavity, each paranasal sinus is lined with ciliated pseudostratified columnar epithelium and is coupled with an ostium, or small boney orifice, that connects each sinus to the nasal cavity of the skull. Functionally, each cavity contributes to reducing the weight of the skull and protecting respiratory openings through the presence of small, finger-like projections known as cilia filtering out any debris that enter the respiratory pathway. In addition to this, a thin layer of mucus is secreted by goblet cells that are integrated into the epithelium, which assist in the immobilization and removal of foreign debris and the preservation of the mucous membrane.
Under normal conditions, the secretions that collect in the paranasal sinuses are drained into the nasal cavity via ostia. But under certain situations, these small orifices can become blocked, resulting in an over-accumulation of the mucus within the chamber. Blockages that occur in the ostia arise due to a number of factors, such as: inflammation of the mucous membrane and polyp growth, abnormalities and/or loss of function in the cilia, initial over-production of mucus secretions, and anatomical abnormalities in the structure of the sinus and ostia. When referring to the development of a local inflammatory response in the mucous membrane of the paranasal sinuses, which is commonly referred to as sinusitis, it is typically stimulated through the adherence, penetration, and proliferation of pathogenic invaders, such as viruses, bacteria, fungi, and superantigens, in the mucous lining and through the inhalation of the allergenic agents, such as pollen and pet dandruff. Upon detection of these foreign entities, an immune response will be initiated. Similar to rhinitis, immunoglobin (IgE) will be released, which will activate neighbouring mast cells, stimulating the release of a number of inflammatory-inducing molecules, such as histamine, leukotriene, and cytokines. Collectively, these molecules will mediate an inflammatory response in the mucous membrane and stimulate the release of additional secretions from the membrane. Inflammation of the mucous membrane can reduce the diameter of the passageway connecting to the ostia, and in conjunction with the polyp growth that is common during nasal inflammation, the passageway can become blocked. In addition to a narrowing of the passageway, the recruitment of prostaglandins and histamines associated with the inflammation will mediate edema, which is an accumulation of inflammatory fluid in the sinuses. This, in conjunction with the absorption of the remaining air in the chamber into the surrounding blood vessels, will create an increase in positive pressure in the sinuses. This accumulation in pressure can compress nearby nerve endings, generating a painful response commonly referred to as a sinus headache. A visual representation illustrating the structural changes that occur in the paranasal sinuses of an individual with sinusitis is provided in Figure 6.
When referring to the diagnostic process, sinusitis is typically detected through a physical examination of the epithelial lining within the nasal pathway. Any tenderness, swelling, or redness that is detected upon examination can be a strong indicator of sinusitis or associated conditions. Other useful modalities include: nasal endoscopy, imagining studies, examination of nasal and sinus cultures, and allergy testing. Nasal endoscopy involves the insertion of a thin, flexible tube-like device equipped with a light and camera into the nostril. This device allows the practitioners to directly monitor the state of the paranasal sinuses without administering any surgical procedures. MRI or CT scans can also be utilized as an effective tool for detecting any abnormalities in the paranasal sinuses through providing an accurate 3-dimensional image of the region. Extracting and examining epithelial tissue from the nasal and parasinal walls can also be an effective approach for determining the etiology of the condition, particularly when the patient isn’t exhibiting any notable improvement when exposed to other available treatment options. According to Hanson, Schmidt, Rosborg and Lund (1995) the extraction of sinus culture via direct sinus puncture is considered to be the gold standard for diagnosing acute sinusitis, producing sensitivity upwards of 82% when detecting C-reactive protein concentrations and erythrocyte sedimentation, two common biomarkers associated with acute sinusitis. Like most conditions that are mediated through allergens, conventional scratch, prick/puncture, intradermal, and patch tests, which involve exposing a section of skin to a variety of suspected allergens and examining the physical changes that occur in the skin, can be an effective approach to utilize.
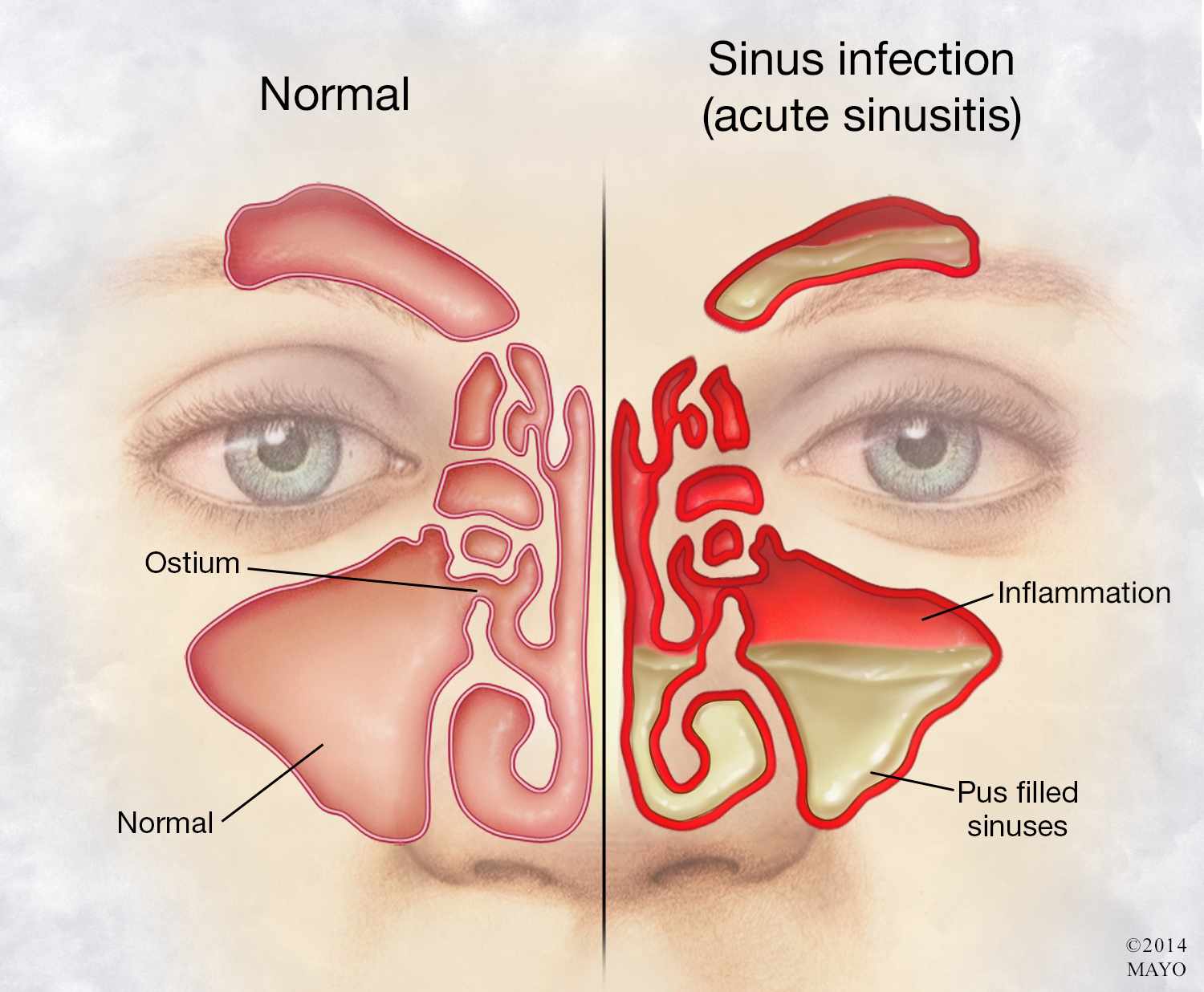
Figure 6. A visual representation of the structural changes that occur in the paranasal sinuses of an individual with acute sinusitis. (Image retrieved from: https://newsnetwork.mayoclinic.org/discussion/mayo-clinic-q-a-chronic-sinusitis-symptoms-often-resemble-a-cold-but-last-for-months/).
Treatment & Surgical Intervention:
With regards to treating acute and chronic sinusitis, there are a variety of possible approaches that can be utilized to address the condition. Various forms of decongestants are available on the pharmaceutical market, such as tablets, solutions, and sprays, which can play a supplementary role in alleviating congestion and removing allergens and pathogens from the nasal cavity and paranasal sinuses. Nasal decongestants have shown to yield the best results with regards to reducing secretions, facilitating drainage, and increasing the overall patency (openness) of the maxillary and frontal ostia due to its ability to penetrate the osteomeatal complex, which is a common channel that provides drainage and ventilation for the frontal and maxillary sinuses, as well as the anterior ethmoid air cells. In addition to this, the usage of non-steroidal anti-inflammatory drugs (NSAIDs) and corticosteroids have also shown to be effective at reducing the local inflammation in the sinuses and alleviating some of the symptoms associated with sinusitis. Some of the common NSAIDs used include: aspirin, acetaminophen, and ibuprofen. Some of the corticosteroids that can be administered via tablet or spray include: fluticasone, budesonide, mometasone, and beclomethasone. If a bacterial infection is the suspected cause of the condition, the prescription of antibiotics has shown to be effective at killing off any microbial agents that are mediating the inflammatory response, such as streptococcus pneumonia. If the bacterium happens to develop resilience to the antibiotic, antimicrobial photodynamic therapy (PDT) can be used to gradually kill off bacteria and lessen bacterial resistance to a given antibiotic through the usage of a low powered laser coupled with a photosensitizer drug. According to Low et al (1997), the adjunct usage of PDT with a variety of antibiotics, such as loracarbef, amoxicillin, and amoxicillin-clavulanate, can exhibit a significant clinical improvement in upwards of 90% of patients in as early as 72 hours following the initial usage of the treatment. If allergens are the etiology (cause) of the condition, the usage of immunotherapy has shown to improve one’s immunological tolerance through incremental exposure to certain allergens. If none of the previously stated treatment approaches have shown to facilitate improvement, then it would be prudent to resort to endoscope sinus surgery (ESS). Similar to a nasal endoscopy, ESS involves the insertion of a thin, flexible tube-like device equipped with a light and camera (endoscope) into the nostrils. Once the ostia of the paranasal sinuses are located, additional instruments are inserted to remove nasal tissue, breakdown nasal polyps, and/or insert small balloon-like structures through the process of balloon sinuplasty into the walls of the passageways that feed into the paranasal sinuses with intent of increasing the functional diameter of each pathway. A visual representation of the associated structures and the equipment utilized in the endoscopic sinus surgery (ESS) is provided in Figure 7.
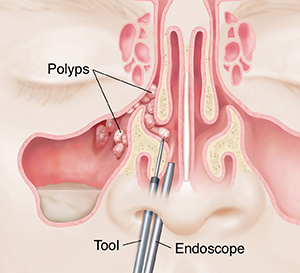
Figure 7. A visual representation of the polyp growth that commonly forms in the paranasal sinuses and respected nasal passageways during sinusitis, and the instruments that are typically utilized to extract these structures during the endoscope sinus surgery (ESS). (Image retrieved from: https://oregon.providence.org/our-services/e/endoscopic-sinus-surgery/).
Adenoiditis
Description:
Adenoiditis is a particular clinical condition that is characterized by the onset of a local inflammatory response in the pharyngeal tonsil (adenoids) facilitated through microbial infection. The infection that occurs in the adenoids can often mediate a hypertrophic response in the tissue, causing the functional diameter of the eustachian tube to shrink. This can impair normal gas exchange, and can sometimes manifest into more severe complications if left untreated.
Symptoms:
- Snoring
- Dry mouth and cracking of lips
- Discoloured discharge of mucus from the nostrils
- Sleep apnea (a condition which involves an obstruction in the neurological signals responsible for regulating breathing patterns during sleep, causing one to spontaneously stop breathing during the sleep cycle)
- Nasal congestion/obstructed nasal sound produced upon speaking
- Swollen glands of the neck
- Ear and sinus infections
Mechanism & Diagnosis:
The pharynx, which is a funnel-shaped passageway that plays in integral role in respiration and digestion through connecting the mouth and nasal cavity to the esophagus and larynx, is commonly divided into three distinct regions. These include the: nasopharynx, oropharynx, and larynogopharynx. A visual representation of the pharyngeal regions is provided in Figure 8. When referring specifically to the nasopharynx, which is located posterior to the nasal fossa of the occipital bone and superior to the soft palate of the back of the nose, it is important in promoting respiratory maintenance while the mouth is closed by connecting the nasal cavity to the orothopharynx, which allows for a continuous exchange of air between the nostrils and lungs. Anatomically, the nasopharynx and orthopharynx are surrounded by a network of lymphatic tissue commonly referred to as the pharyngeal lymphoid ring, or Waldeyer’s lymphatic ring. When looking at the superior aspect of the network along the posterior pharyngeal wall, there is a condensed cluster of lymphoepithelial tissue embedded beneath the cilia and mucus lining the wall known as the pharyngeal tonsil (adenoids). This tissue is composed of: epithelial cells, lymphocytes, macrophages, and dendritic cells, and is abundant in T-lymphocytes. Functionally, T-lymphocytes assist in the initiation of an immunological response, the activation and recruitment of white blood cells, such as cytotoxic T cells and marcophages, the destruction of infected cells, and the development of immunological memory through the production of memory T cells.
Under certain conditions, microbial agents, such as the adenovirus and enterovirus, will begin to adhere to and infect the deep crypts in the palatin and pharyngeal tonsils. This will mediate an immunological response, which involves a number of key processes such as the recruitment of white blood cells to the region of infection and the onset of a local inflammatory response. The infection and inflammation of the palatin and pharyngeal tonsils will cause the tissue to engage in a hypertrophic response, reducing the diameter of the pathway between the middle ear and nasopharynx, which is commonly referred to as the eustachian tube. This inflammatory condition is referred to adenoiditis, and can play a major role in obstructing airflow across the eustachian tube, which can manifest into more severe respiratory conditions such as sleep apnea. A visual representation of the infected pharyngeal tonsils (adenoids) during adenoiditis is provided in Figure 9.
When referring to the diagnostic process for adenoiditis, there are a number of approaches that are commonly utilized among practitioners when attempting to detect the condition. Physical examinations and the collection of medical history are always important preliminary steps to take when determining the location of the inflammation and the etiology (cause) of the condition. Many practitioners will commonly swab the region to provide an analytical breakdown of the microbial composition of the area. Another effective method of physically examining the nasopharynx is through the usage of a flexible, fibroptic scope (endoscope). According to the research, this is considered to be the most accurate diagnostic modality due to the direct observation of the region that is provided with the instrument. Other diagnostic approaches that are commonly utilized include: blood tests, which will provide a representation of the microbial composition and white blood cell concentration in the blood, and image screening through the usage of CT, MRI, and X-rays to develop an accurate image of the location and severity of the condition.
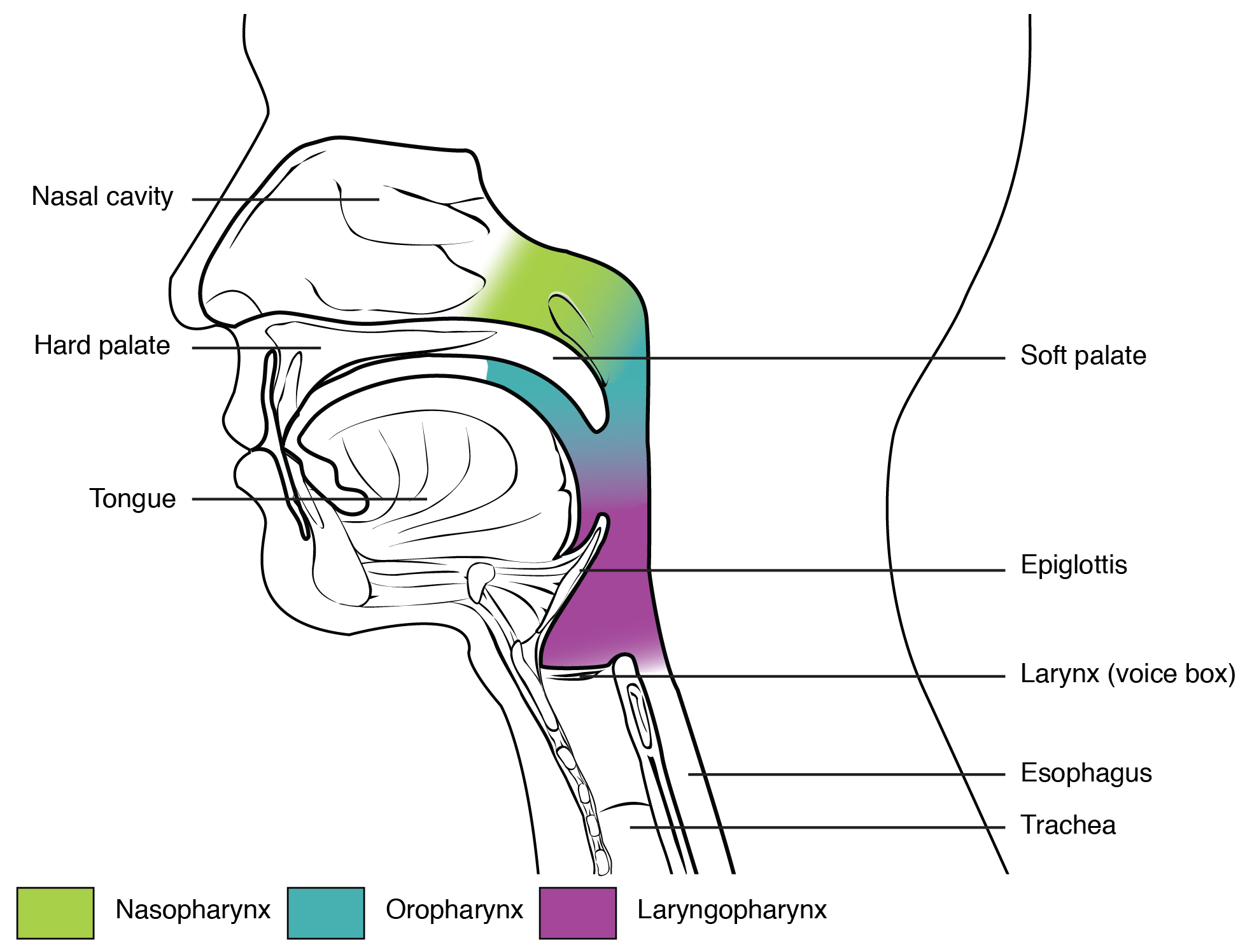
Figure 8. A visual representation of the pharyngeal regions and associated structures. (Image retrieved from: https://pressbooks.bccampus.ca/aandpfundamentals/wp-admin/post.php?post=4394&action=edit).
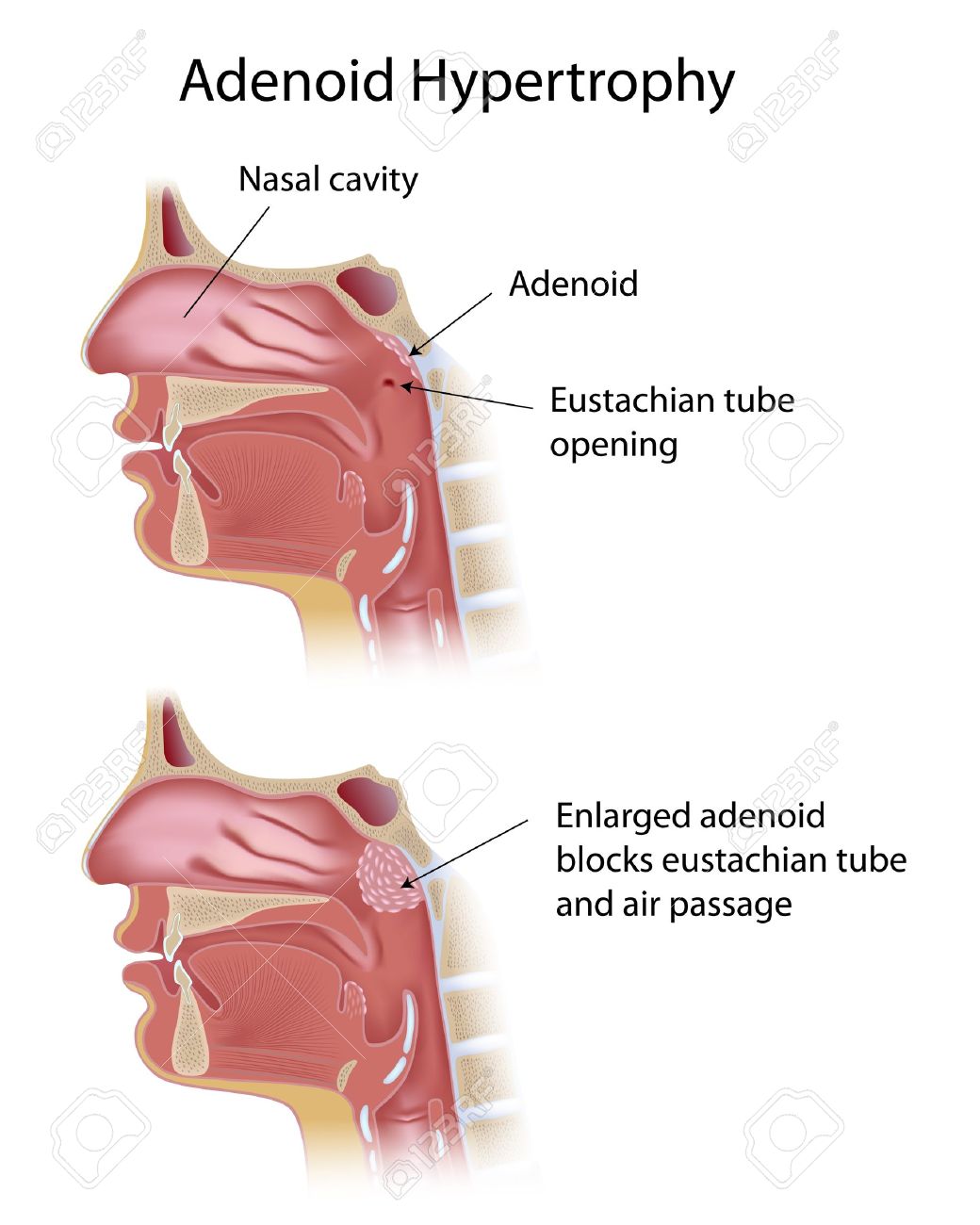
Figure 9. A visual representation of the structural changes that occur in the pharyngeal tonsils (adenoids) in an individual inflicted with adenoiditis. (Image retrieved from: https://www.practo.com/health-wiki/adenoiditis-symptoms-complications-and-treatment/266/article).
Treatment & Surgical Intervention:
There are a number of treatment modalities that are commonly used when addressing adenoiditis. If bacterial infection is the suspected cause of the condition, prescribing antibiotics can be an effective approach for gradually killing off any harmful bacterial populations that are responsible for mediating the condition. In conjunction with antibiotics, prescribing non-steroidal anti-inflammatory drugs (NSAIDs) or corticosteroids can be useful for reducing the inflammatory response within the infected tissue. If antibiotics fail to provide any improvement, the next logical step would be to have to have the nasopharyngeal tonsil surgically removed. The process of accomplishing this is referred to as adenoidectomy. There are many variations of adenoidectomy, each utilizing different instruments and techniques to accomplish the common goal of extracting the infected adenoids from the pharyngeal wall. According to the literature, the most effective approaches to adenoidectomy typically involve the usage of a transoral (70 degree) or transnasal (0 degree) endoscope, coupled with a straight blade or curved blade microdebrider, followed up with digital palpation of the nasopharynx following the surgical removal of the adenoids. A visual representation of the adenoidectomy procedure is provided in Figure 10. This particular approach provides a high-quality image of the adenoids, allowing for a more controlled and comprehensive removal of the infected tissue. Besides providing a quality extraction, this approach is also good at preserving the integrity of the surrounding structures, such as the pharyngeal muscles, reducing the risk of any post-operative medical complications.
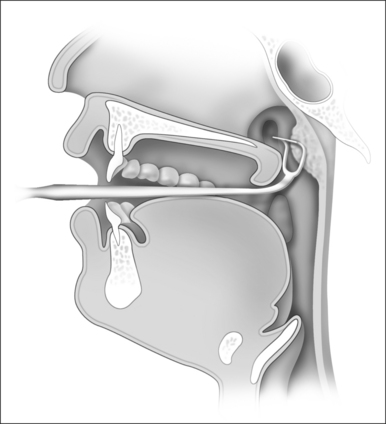
Figure 10. A visual representation of a standard adenoidectomy procedure accomplished with a transoral endoscope coupled with a straight blade microdebrider. (Image retrieved from: https://pocketdentistry.com/current-techniques-of-adenoidectomy/).
References
Acute Sinusitis. (2018, February 6). Mayo Clinic. Retrieved from: https://www.mayoclinic.org/diseases-conditions/acute-sinusitis/symptoms-causes/syc-20351671
Adenoiditis: An Infection of Your Infection-Fighting Tissue. (2016, January 6). Healthline. Retrieved from: https://www.healthline.com/health/adenoiditis
Beule, A. (2010). Physiology and Pathophysiology of Respiratory Mucosa of the Nose and the Paranasal Sinuses. GMS Current Topics in Otorhinolaryngology, Head and Neck Surgery, 9. doi: 10.3205/cto000071
Brambilla, I., Pusateri, A., Pagella, F., Caimmi, D., Caimmi, S., Licari, A & Marseglia, G. (2014). Adenoids in Children: Advances in Immunology, Diagnosis, and Surgery. Clinical Anatomy, 27(3), 346-352. doi: https://doi.org/10.1002/ca.22373
Chronic Sinusitis. (2018, March 3). Mayo Clinic. Retrieved from: https://www.mayoclinic.org/diseases-conditions/chronic-sinusitis/symptoms-causes/syc-20351661
Church, M & Scadding, G. (2018). Allergic Rhinitis: Impact, Diagnosis, Treatment and Management. Lung Cancer, 15, 5. Retrieved from: https://www.pharmaceutical-journal.com/research/review-article/allergic-rhinitis-impact-diagnosis-treatment-and-management/20201509.article
Endoscope Sinus Surgery. (2015, February 17). American Rhinologic Society. Retrieved from: http://care.american-rhinologic.org/ess
Hansen, J., Schmidt, H., Rosborg, J & Lund, E. (1995). Predicting Acute Maxillary Sinusitis in a General Practice Population. Bmj, 311(6999), 233-236. doi:https://doi.org/10.1136/bmj.311.6999.233
Hay Fever. (2018, August 1). Mayo Clinic. Retrieved from: https://www.mayoclinic.org/diseases-conditions/hay-fever/symptoms-causes/syc-20373039
Kouzegaran, S., Zamani, M., Faridhosseini, R., Rafatpanah, H., Rezaee, A., Yousefzadeh, H & Tehrani, H. (2018). Immunotherapy in Allergic Rhinitis: It’s Effect on the Immune System and Clinical Symptoms. Open Access Macedonian Journal of Medical Sciences, 6(7), 1248. doi: 10.3889/oamjms.2018.264
Lieberman, P & Anderson, J. (2007). Allergic Diseases: Diagnosis and Treatment. Retrieved from: https://link-springer-com.ezproxy.viu.ca/content/pdf/10.1007%2F978-1-59745-382-0.pdf
Low, D., Desrosiers, M., McSherry, J., Garber, G., Williams, J., Rémy, H & Craft, C. (1997). A Practical Guide for the Diagnosis and Treatment of Acute Sinusitis. Canadian Medical Association. Journal, 156(6), S1. Retrieved from: https://search-proquest-com.ezproxy.viu.ca/docview/1942177773/fulltext/881C04A3CD594D1DPQ/1?accountid=12246
Marieb, E., Mallatt, J & Wilhelm, P. (2005). Human Anatomy, San Fransico, CA: Pearson Education, Inc.
Min, Y. (2010). The Pathophysiology, Diagnosis and Treatment of Allergic Rhinitis. Allergy, Asthma & Immunology Research, 2(2), 65-76. doi:https://doi.org/10.4168/aair.2010.2.2.65
Moore, K., Dalley, A & Agur, A. (1999). Clinically Oriented Anatomy. Baltimore, Maryland: Lippincott Williams & Wilkins.
