Thorax
Organs and Special Regions
The Mediastinum
What is the Mediastinum?
The mediastinum is the central compartment of the chest located deep to the thoracic cage, superior to the diaphragm and sits medial to the two pleural cavities of the lungs. It contains the heart and all thoracic viscera minus the lungs.
Divisions of the mediastinum:
The mediastinum consists of two regions the superior and inferior region. The inferior region can be divided into three divisions: anterior, middle, and posterior.
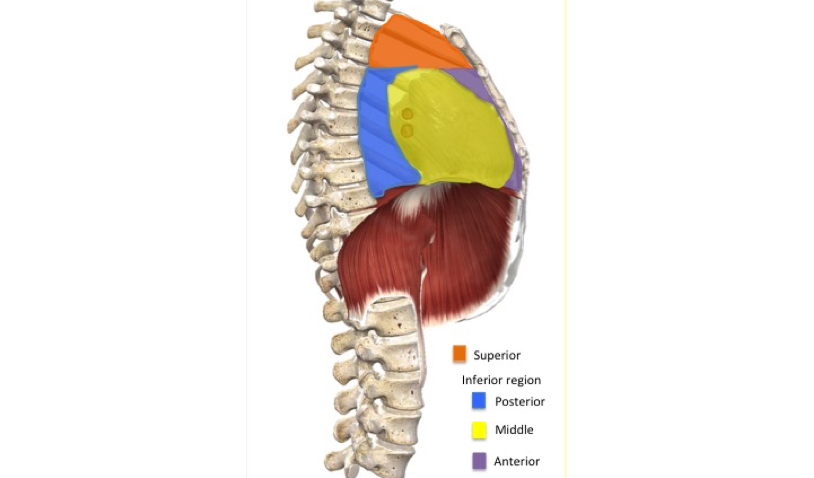
The superior region is located above the level of the pericardium. The superior border is outlined by the thoracic inlet, the anterior boarder by the manubrium of the sternum, the posterior boarder by the vertebral bodies of T1-T4 and the lateral boarder by the pleurae of the lungs. The superior region of the mediastinum contains the thymus, great vessels related to the heart, trachea and the esophagus.
The inferior region of the mediastinum contains three divisions, anterior, posterior and middle.
The anterior division is located between the sternum and the pericardium. The boarders of this region include, the lateral that is marked by the mediastinal pleura, the anterior by the body of the sternum, posterior by the pericardium and the inferior border of the anterior division by the diaphragm. The only thing found in this division of the mediastinum is the thymus.
The posterior division is located behind the pericardium and contains the esophagus and the thoracic aorta. The borders of this region include, the lateral that is marked by the mediastinal pleura, the anterior by the pericardium, the posterior by T5-T12 vertebrae, the superior by the T4 vertebrae to manubrium of the sternum and the inferior boarder by the diaphragm.
The middle division contains the pericardium, the heart, main bronchi and other structures at the root of the lungs. This division is determined by the anterior boarder at the anterior margin of the pericardium, the posterior boarder at the posterior boarder of the pericardium, the lateral boarder at the mediastinal pleura, the superior boarder at the sternal angle to T4 vertebrae and inferiorly by the diaphragm.
Muscles…
Superior region:
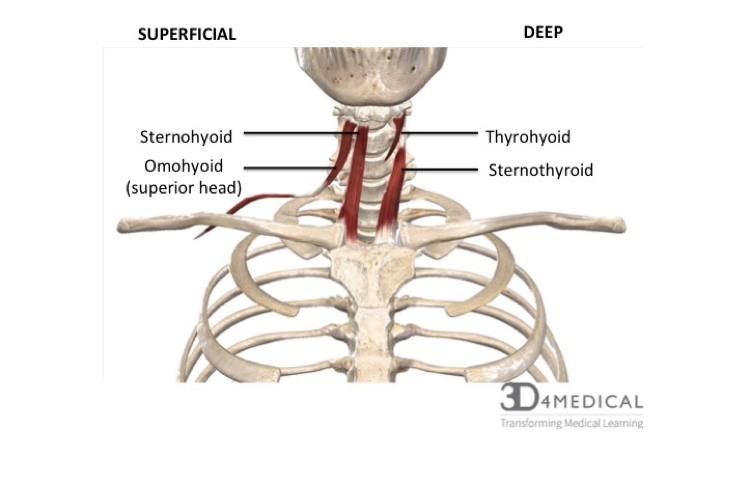
The Sternohyoid and Sternothyroid muscles are found in the superior region of the mediastinum. These muscles originate from the posterior surface of the manubrium and are part of the infrahyoid muscle group of the neck.
Joints, ligaments and connective tissue:
The superior region and the anterior division of the mediastinum contain the Sternopericardial ligaments that are responsible for tethering the pericardium to the sternum.
The posterior division contains the vetrebropericardial ligaments that are responsible for tethering the pericardium to the vertebrae.
The inferior region of the mediastinum contains the phrenicopericardial ligament that is responsible for tethering the pericardium to the diaphragm.
Organs….
The middle division:
This includes the heart that will be covered in the next chapter. https://pressbooks.bccampus.ca/advancedanatomy1sted/chapter/the-heart/
Posterior division:
Esophagus:
The esophagus passes into the posterior division of the mediastinum from the superior mediastinum and descends posteriorly to the arch of the aorta and the heart. The esophagus is initially positioned to the right but deviates to the left as it moves downwards and exits the mediastinum via the esophageal hiatus of the diaphragm.
Blood vessels…
Superior region:
The superior region of the mediastinum contains blood vessels such as the arch of aorta and the superior vena cava.
The arch of the aorta has three main blood vessels branches. The first blood vessel that branches off the aortic arch on the right side is called the brachiocephalic artery and it splits into two arteries, the right common carotid and the right subclavian. The right common carotid artery supplies blood to the right side of the head and neck. The right subclavian artery supplies blood to the right upper limb. The second blood vessel that branches off in the middle of the arch on the left hand side is the left common carotid artery that supplies blood to the left side of the head and neck. The blood vessel that branches off the aortic arch on the left side is the left subclavian artery and is responsible for supplying blood to the left upper limb.
The superior vena cava returns deoxygenated blood from the head, neck, upper limbs and thorax to the right atrium of the heart. The left superior intercostal vein receives blood from the 2nd and 3rd intercostal vein and drains into the left brachiocephalic vein. The superior intercostal vein drains the blood from the first intercostal space directly into the brachiocephalic veins. The brachiocephalic veins drain deoxygenated blood from upper limbs into the superior vena cava where it is then returned to the right atrium.
Middle Division:
The middle division of the mediastinum contains blood vessels such as the ascending aorta, pulmonary trunk, and the superior vena cava. The ascending aorta is the first part of the aorta that arises from the aortic orifice. It moves upwards and exits the fibrous pericardium while entering the superior mediastinum, where it then becomes the aortic arch. The ascending aorta gives rise to two branches, the left and right coronary arteries. The pulmonary trunk comes off of the right ventricle and extends upwards where it branches into the left and right pulmonary arteries that carry deoxygenated blood to the lungs.
Posterior division:
The posterior division of the mediastinum contains blood vessels such as the thoracic/descending aorta, the posterior intercostal arteries, bronchial arteries, esophageal arteries and the superior phrenic arteries. The thoracic/descending aorta is a continuation of the aorta arch beginning at the lower edge of the T4 vertebra and descends through the posterior mediastinum to the left of the vertebrae. As the thoracic aorta descends it becomes more medially located as it moves. At the inferior border of T12 the thoracic aorta becomes the abdominal aorta and passes through the aortic hiatus of the diaphragm. The thoracic aortia gives rise to many branches of blood vessels such as, the posterior intercostal arteries, bronchial arteries esophageal arteries and the superior phrenic arteries.
The posterior intercostal arteries are paired parietal branches that consist of nine paired branches. They are responsible for supplying the intercostal spaces, except the first two. The posterior intercostal arteries pass posteriorly and laterally, in parallel with the ribs.
The bronchial arteries are paired visceral branches, left and right. The left bronchial arteries always arise directly from the thoracic aorta where as the right usually branch indirectly from a right posterior intercostal artery. These arteries are responsible for supplying the tracheobronchial tree.
The esophageal arteries are unpaired visceral branches arising from the anterior aspect of the aorta. They usually consist of 2-5 arteries and are responsible for blood supply to the esophagus.
The superior phrenic arteries arise from the anterior aspect of the thoracic aorta at the aortic hiatus and are responsible for supplying blood to the superior aspect of the diaphragm.
Lymph…..
Posterior division:
The posterior division of the mediastinum contains the thoracic duct, which is the largest lymphatic vessel in the body. The thoracic duct allows return of lymph from most of the body with the exception of the right superior quadrant, into the venous system. The duct originates from the cisterna chyli in the abdomen and enters the mediastinum through the aortic hiatus where it ascends to lie directly anterior to the T6-T12 vertebrae. From there it deviates to the left as it ascends into the superior mediastinum. Although the thoracic duct is located in the posterior mediastinum, it receives lymphatic drainage from the intercostal spaces and neighbouring anatomical structures.
Middle division:
The middle division of the mediastinum contains the tracheobronchial lymph nodes. These nodes form from the gathering of bronchial nodes within the hila of the lungs and are associated with the trachea and bronchi of the respiratory tract.
Nerves…..
Middle division:
The middle division of the mediastinum contains the cardiac plexus, which is a network of nerves located at the base of the heart, containing sympathetic and parasympathetic fibres. The sympathetic nerves are derived from the T1-T4 segments of the spinal cord whereas the parasympathetic innervation is supplied by the vagus nerve. The cardiac plexus can be subdivided into superficial and deep components that form the superficial and deep cardiac plexuses found in the superior mediastinum. The cardiac plexus originates from the superior, middle and inferior cardiac ganglion. The superior plexus sits between the aortic arch and right pulmonary vein where the deep plexus lies on the surface of the trachea at the point of bifurcation.
Superior and middle region:
The phrenic nerves are mixed nerves that provide motor innervation to the diaphragm and can be found in both the superior and middle regions of the mediastinum. The phrenic nerves arise in the neck and enter the superior mediastinum lateral to the great vessels where they then descend anteriorly into the middle mediastinum, passing anteriorly to the hilum of the lungs.
Posterior division:
The posterior division of the mediastinum contains the esophageal plexus as well as the thoracic sympathetic trunk. The esophageal plexus is a network of nerves surrounding the esophagus as it descends and is comprised of branches from the left and right vagus nerves. Immediately above the diaphragm, the fibres of the plexus converge to form the anterior vagal trunk and posterior vagal trunk where they travel along the surface of the esophagus as it exits the thorax.
The thoracic sympathetic trunks lies within the posterior mediastinum and are made up of paired bundles of nerves that extend from the base of the skull to the coccyx. They run bilaterally to vertebral bodies along the entire length of the vertebral column where they gives rise to the lower thoracic splanchnic nerves, which innervate the viscera of the abdomen.
Clinical portion……
Anterior mediastinum:
Clinical problems that are associated with the anterior division of the mediastinum include, substernal thyroid goiters, lymphoma, thymoma, and teratoma. Substernal thyroid goiters are caused by an abnormal growth of the thyroid gland and lead to the compression of the trachea and esophagus resulting in a choking sensation or cough. Mediastina lymphoma or lymphoma in general is a cancer that effects the lymphocytes which are present in the thymus that is located in the anterior mediastinum. Thymoma is a tumor originating from the epithelial cells of the thymus that can be benign or malignant. Mediastinal teratoma usually occurs within or near the thymus gland and are germ cell tumours arising from ectopic pluripotent stem cells that failed to migrate from yolk endoderm to the gonad.
Middle division:
Clinical problems associated with the middle division of the mediastinum include but are not limited to, lymphadenopathy. Lymphadenopathy is a disease of the lymph nodes that is caused by abnormal size, numbers or consistency of the lymph nodes.
Posterior division:
Clinical problems associated with the posterior mediastinum include neurogenic tumors. Neurogenic tumors originate from either the nerve sheath, mostly benign, or elsewhere, mostly malignant. These are the most common tumors of the mediastinum.
Other conditions associated with the mediastinum:
Mediastinitis is an inflammation of the tissues in the mediastinum and can be a life threatening condition if treated improperly. Mediastinitis usually occurs due to a tear in the esophagus or after chest surgery.
Pneumomediastinum is caused by an abnormal presence of air or gas in the mediastinum. This air or gas can originate from the lungs, trachea, central bronchi, or the esophagus.
A widened mediastinum is a mediastinum with a width greater than 6-8cm depending on the type of x-ray. A widening of the mediastinum can be caused by numerous conditions, such as tumors, aortic aneurysm, aortic dissection, aortic unfolding or enlarged lymphoid mass to name a few. Most cases require immediate attention.
The Respiratory System
Introduction:
The respiratory system works seamlessly with the circulatory system to transport oxygen and carbon dioxide throughout the body. With each inhalation, oxygen and other gases are brought into the lungs and with each exhalation, carbon dioxide is expelled. Each and every cell in the human body requires adenosine triphosphate (ATP), which is a form of energy the body is able to use. For ATP to be produced, the oxidative stages of cellular respiration use oxygen as a reactant, and carbon dioxide is formed as a waste product. A buildup of this by-product is the primary driving factor behind respiration as this can, in turn, alter the pH of the blood. The respiratory system also has a role in producing sounds for speech, sensory functions such as discerning odours, and the physical movement of air in and out of the body. This section will cover the structure of the respiratory system, including the muscles of respiration, and will also focus on clinical conditions affecting this system and impeding proper function.
Organs and Structures of the Respiratory System:
The respiratory system is comprised of two different areas: a conducting zone and a respiratory zone. The conducting zone allows for a pathway for air to travel but is not directly involved in the process of gas exchange, whereas the respiratory zone is where gas exchange occurs.
The Conducting Zone: This area provides a passageway for air to flow in and out of the body. It also has the role of warming and humidifying air being inhaled, while simultaneously removing debris and pathogens. Its structures include the nose, pharynx, larynx, trachea, and the bronchial tree.
The nose has mucous membranes along with accessory structures such as sebaceous glands and hair follicles lining the nasal cavities. These serve to remove large airborne particles from incoming air which acts as a defensive mechanism along with secreting an enzyme with antibacterial properties by the name of defensins. Also housed within the nasal cavity is olfactory epithelium, which allows for the perception of odors, and respiratory epithelium which is made up of pseudostratified ciliated columnar epithelium. One unique feature about the epithelial lining, is that is has specialized mucus-producing goblet cells. Debris gets stuck in the mucus and the cilia moves the mucus out of the nasal passageways into the throat where it can be swallowed or coughed up.
The pharynx can be subdivided into 3 sections: the nasopharynx, the oropharynx and the laryngopharynx.
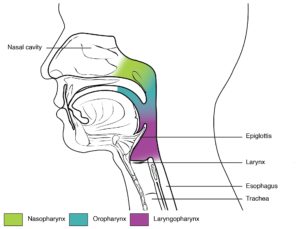
Figure 1: The Conducting Zone and Subdivisions of the Pharynx
Posterior and inferior to the laryngopharynx lies the larynx which controls the quantity of air moved in and out of the body. The larynx is comprised of 3 pieces of cartilaginous tissue: the thyroid cartilage, the cricoid cartilage, and the epiglottis which lies directly superior to the trachea. The epiglottis intercepts foods and liquids to prevent them from entering the trachea.
The trachea is composed of C-shaped sections of hyaline cartilage that serves to support the airway and prevent it from collapsing maintaining constant respiratory function. It is assisted by the trachealis muscle, which connects the sections of cartilage, can be contracted to expel air forcefully from the airways.
The bronchial tree begins where the trachea splits into two left and right primary bronchi at a very sensitive structure made up of nervous tissue called the carina. If a foreign object comes in contact with the carina, a violent coughing reflex occurs in attempt to expel the object from the airways. The primary bronchi pass through the only opening into the lungs where blood vessels, lymphatic vessels, and nerves also enter in an area called the hilum. Within the lung, the left and right primary bronchi divide into smaller branches called secondary bronchi and tertiary bronchi. Each of these structures is supported by rings of cartilage. From the tertiary bronchi, even smaller airways called bronchioles branch off which no longer contain cartilage rings for support, but instead are lined with smooth muscle to increase or decrease airflow accordingly. The bronchioles divide further into terminal bronchioles which then lead into the structures called respiratory bronchioles associated with gas exchange in the respiratory zone.
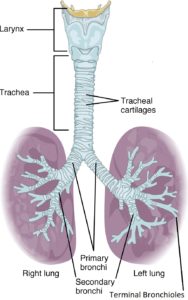
Figure 2: Conducting Zone from Larynx to Terminal Bronchioles
The Respiratory Zone:
Respiratory bronchioles conduct air into clusters of alveoli through alveolar ducts. The Alveolus is a spherical sac that are elastic in nature, allowing them to stretch and expand with incoming air flow, increasing the surface area to allow for maximum gas exchange. Alveolar sacs are groups of alveoli connected through alveolar pores which allow for the controlled, equal air pressure within the respiratory zone.
Figure 3: The Respiratory Zone
Within the alveolus there are three types of cells: Type I Pneumocytes which make up the structural wall of the alveolus, it is a single cell thick which is permeable to gases. Type II Pneumocytes secrete pulmonary surfactant, which reduces surface tension within the alveolus and prevents these delicate structures from collapsing if there is moisture in the lungs. Alveolar macrophages assist the immune system by removing airborne pathogens and debris that have made their way down the respiratory tract into the alveoli.
The Lungs:
The lungs are housed within the thoracic cavity and are enveloped by the pleurae which is a bilayer of serous membrane with a thin layer of serous fluid that lubricates and reduces friction between the organs and the ribcage during movement and respiration as well as having the function of increasing surface tension between the lung and the thoracic wall, which helps with the positioning of the organs as well as aiding in respiration as the thoracic cavity expands and compresses. The layer directly in contact with the lung is called the visceral pleura, and the layer in contact with other structures such as the ribs, mediastinum, and diaphragm, is called the parietal pleura. The lungs are bordered inferiorly by the diaphragm, which is the primary muscle of inspiration marking the division between the thoracic cavity and the abdominopelvic cavity. The external intercostal muscles also assist in respiration by elevating the ribs, while the internal intercostal muscles and the innermost intercostal muscles depress the ribs in expiration.
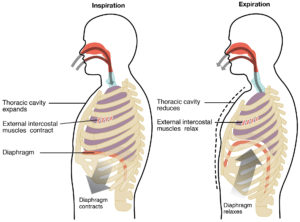
Figure 4: The Muscles of Respiration
The right lung has 3 lobes: a superior lobe, an inferior lobe, and a middle lobe separated by a horizontal fissure and an oblique fissure respectively. The left lung has a unique feature called the cardiac notch which is the concave area allowing room for the heart. The left lung has only 2 lobes: a superior lobe and an inferior lobe separated by an oblique fissure.
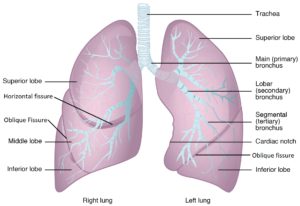
Figure 5: Gross Anatomy of the Lungs
The Pulmonary Circuit:
Deoxygenated blood from the system flows into the right atrium of the heart through the superior and inferior vena cavae, which then is pumped into the right ventricle passing through the right atrioventricular valve also known as the tricuspid valve. It then exits the right ventricle through the pulmonary semilunar valves and travels through the pulmonary trunk leaving the heart in the pulmonary arteries. These arteries divide into smaller arterioles and eventually capillaries and capillary beds surrounding the alveolar sacs in the lungs creating what is called the respiratory membrane. These single-cell-thick blood vessels allow for gas exchange through simple diffusion within the alveoli, retrieving oxygen and removing carbon dioxide. These capillary beds join to form venules, which become veins, and conjoin to form the pulmonary veins that carry oxygen-rich blood back to the heart, entering the left atrium. The blood then travels through the left atrioventricular valve, also known as the bicuspid or mitral valve, into the left ventricle. The left ventricle contracts, and blood exits through the aortic semilunar valve into the aorta to disperse oxygen rich blood to the rest of the body. Once it has reached all the tissue to drop off oxygen and pick up carbon dioxide, it returns back to the heart via the venous system, entering the right atrium once again through the superior and inferior vena cavae.
Pulmonary Innervation:
The respiratory system is under both parasympathetic and sympathetic nervous control. Bronchoconstriction, or the narrowing of the bronchioles is stimulated by parasympathetic motor nerve fibers, and bronchodilation, which is the expansion of the bronchioles, is influenced by sympathetic motor nerve fibers. Respiratory reflexes like coughing is under autonomic nervous control as well to maintain and regulate both oxygen and carbon dioxide levels in the body accordingly. The respiratory system is innervated by the pulmonary plexus with nerve fibers arising from the Vagus nerve (Cranial Nerve X) and ganglia from T1-T5.
Embryonic Development of the Respiratory System:
The respiratory system starts to develop within the fetus approximately around week four. Olfactory pits begin to form from ectodermal tissue, which will eventually form the nasal cavity. These olfactory pits fuse with the endodermal tissue of the pharynx, forming the opening of the conducting zone of the respiratory tract. Around week 4, the lung bud also begins to form, which is comprised of endodermal tissue from the foregut which is located inferiorly to the pharangeal pouches. The lung bud develops an extension from it as it grows called the laryngotracheal bud which eventually forms the trachea on one end, and the other end forms bronchial buds. Around week 7, bronchial buds begin to develop and increase in size and diameter into bronchi, which branch. Vascularization and the beginnings of alveolar structures commence formation in the sixteenth week. Also occurring in week 16, the respiratory bronchioles start to form and complete their development by week 19. Type I pneumocytes and Type II pneumocytes start to differentiate also around week 19, with type II pneumocytes secreting small amounts of surfactant. Fetal breathing movements may occur within week 20-21, which are muscle contractions causing the inhalation of amniotic fluid and exhalation of surfactant and mucus. This is to perhaps prepare the infant for breathing movements after birth however, it is not exactly clear if this is the only cause. Weeks 24 to term involve the development of the alveoli, (however they are not structurally complete and functional until the child is around 8 years old) and more surfactant production occurs. The respiratory membranes continue to develop for extensive gas exchange. An important milestone occurs at week 28, where the baby has sufficient formations of alveolar precursors to allow the child to breathe independently if born prematurely. After the child is born, the first inhalation serves to inflate the lungs, which is dependent on the presence of pulmonary surfactant. The first inspiration occurs typically within ten seconds of birth.
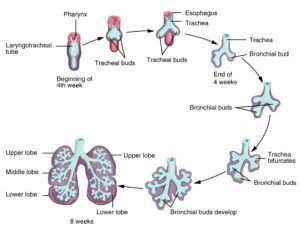
Figure 6: Embryological Development of the Respiratory System: Weeks 4-8

