Lower Limb
Special Anatomical Regions
The Femoral Triangle
The femoral triangle is one of the two of several special anatomical regions of vulnerability in the body in the lower limb. With so many little things to remember in the anatomy of the human body, it becomes tedious to learn and remember everything! However, an easy way to remember the orientation of the contents within the femoral triangle it is to recite this mnemonic: “We NAVI-gate the femoral triangle from lateral to medial” N for nerves, A for Arteries, V for Veins, and I for inguinal lymph nodes. Additionally, for all special anatomical regions of vulnerability (i.e., triangles of the neck, axilla, cubital fossa, femoral triangle, and popliteal fossa) another handy mnemonic to include in one’s arsenal is “NAVEL” N for nerves, A for arteries, V for veins, E for empty space, L for lymph, as all of these regions consist of these contents.
Borders and Contents of the Femoral Triangle
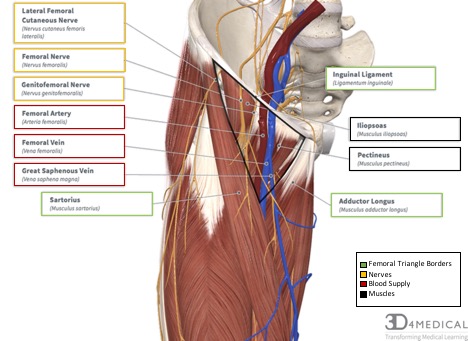
The femoral triangle is a junctional region of vulnerability between the trunk and the lower limb that receives its triangular name from the formation of its triangular fascial space in the superior anterior third of the thigh. It appears as a triangular depression inferior to the inguinal ligament when the thigh is flexed, abducted, and laterally rotated. The femoral triangle is bordered superiorly by the inguinal ligament, medially by the adductor longus muscle, and laterally by the sartorius muscle (see figure 1).
The femoral triangle shape is compared to an upside down, triangle. It has a base that is located superiorly (inguinal ligament) and an apex inferiorly that is formed by the sartorius muscle (lateral border) crossing the adductor longus muscle (medial border). The roof of the femoral triangle is formed by the fascia lata and cribriform fascia, subcutaneous tissue, and skin. While the muscular floor of the femoral triangle is formed from lateral to medial by iliopsoas (Iliacus muscle and psoas major muscle) and pectineus muscle.
Borders:
- Inguinal Ligament (Superior)
- Sartorius (Lateral)
- Adductor Longus (Medial)
Floor: From lateral to medial:
- iliopsoas (Iliacus muscle and Psoas Major muscle)
- Pectineus muscle.
Roof: Is formed by:
- fascia lata and cribriform fascia
- subcutaneous tissue
- skin
Nerves (Lateral to Medial)
Lateral Femoral Cutaneous Nerve (Lateral): Crosses the lateral corner of the triangle and supplies the skin on the lateral part of the thigh (see figure 2). It arises from the lumbar plexus and contains its fibers from the second and third lumbar nerves to supply the skin of the anterior and posterior surface of the thigh.
Femoral Nerve (Intermediate): Lies within the groove between the Iliacus and psoas major muscles (see figure 2). It arises from the ventral rami of the spinal nerves L2-L4. It supplies the quadriceps muscles, sartorius muscle, illiacus muscle, and pectineus muscle, as well as the skin of the anterior thigh. The femoral nerves contain divisions including the: saphenous nerve, nerves to the anterior compartment of the thigh, and the anterior branches cutaneous branches.
Femoral Branch of Genitofemoral Nerve (Medial): Runs in the lateral compartment of the femoral sheath and the supplies the majority of the skin over the femoral triangle (see figure 2). It arises from the ventral rami of spinal nerves L1-L2 and supplies the skin of the proximal medial thigh and the labia majora, or the anterior scrotum, as well as the cremaster muscle.
Artery
The femoral artery is the “chief artery” to the lower limb and is the distal continuation of the external iliac artery. The femoral artery begins at the inguinal ligament as it enters at the midway point between the anterior superior iliac spine and the pubic symphysis. As the femoral artery passes the inguinal ligament it lays lateral to the femoral vein. As the femoral artery descends it lays posteriorly to the fascia lata and on the neighboring borders of the iliopsoas and pectineus muscles that form the floor of the femoral triangle. It enters the adductor canal deep to the sartorius at the apex of the femoral triangle. The femoral artery exits the adductor canal as it passes through the adductor hiatus and becomes the popliteal artery.
Veins
The femoral vein is the proximal continuation of the popliteal vein after it passes through the adductor hiatus as it ascends through the adductor canal. The femoral vein lies posterior and lateral to the femoral artery (see Figure 1). The femoral vein enters the femoral sheath lateral to the femoral canal and ends posteriorly to the inguinal ligament, where it becomes the external iliac vein. In the inferior portion of the femoral triangle, the femoral vein receives drainage from the deep vein of the thigh, the great saphenous vein, circumflex veins, and veins corresponding to the femoral artery. The deep vein of the thigh is formed by the union of three or four perforating veins and enters the femoral vein approximately 8 cm inferior to the inguinal ligament and approximately 5 cm inferior to the termination of the great saphenous vein.
Empty Space is an important space that does not contain any structures.
Lymphatic
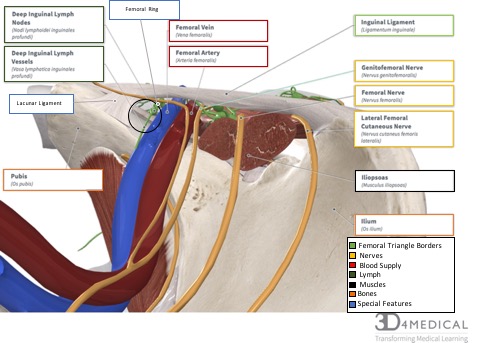
Deep inguinal lymph nodes and vessels cross into the femoral triangle at the medial corner through the femoral ring (see figure 3).
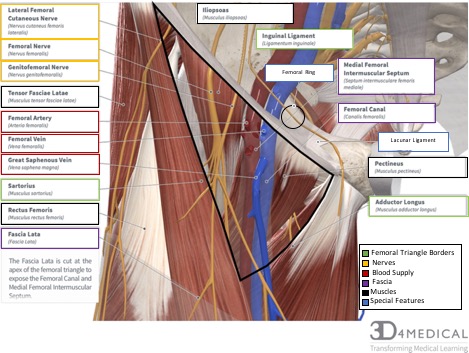
Femoral canal
Of the three compartments within the femoral sheath, the femoral canal is the smallest. The canal is cone-shaped and is approximately 1.25 cm that lies between the medial edge of the femoral sheath and the femoral vein (see figure 3). The canal extends distally to the level of the proximal edge of the saphenous opening and allows the femoral vein to expand when venous return from the lower limb is increased. Additionally, the femoral canal contains connective tissue, fat, a few lymphatic vessels, and sometimes a deep inguinal lymph node (i.e., Cloquet’s node) The base of the femoral canal is formed by the femoral ring. The femoral ring is the small proximal opening of the femoral canal (approximately 1 cm wide) and is closed by extraperitoneal fatty tissue that forms the femoral septum. The femoral septum is penetrated by lymphatic vessels connecting the inguinal and external iliac lymph nodes (see figure 3). The structures that form the boundaries of the femoral ring are as follows:
- Laterally, the partition between the femoral canal and femoral vein
- Posteriorly, the superior ramus of the pubis covered by the pectineus and its fascia
- Medially, the lacunar ligament
- Anteriorly, the medial part of the inguinal ligament
Adductor Canal (Subsartorial or Hunter’s Canal):
The adductor canal is an aponeurotic tunnel in the middle third of the thigh, extending from the apex of the femoral triangle to the opening of the adductor magnus tendon, known as the adductor hiatus. The adductor canal is the space in the middle third of thigh between vastus medialis and the adductor muscles, which is then covered and converted into a tunnel by the overlapping sartorius muscle. The adductor canal provides an intermuscular pathway in which the femoral vessel proceed through to reach the popliteal fossa and become the vessels of the popliteal. The adductor canal contains the following:
- Femoral artery and vein
- Saphenous nerve
- The nerve to vastus medialis
Additionally, the adductor canal is enclosed by the following:
- Anteriorly and laterally by vastus medialis
- Posteriorly by adductor longus and adductor magnus
- Medially by sartorius
Clinical Significance
While in hip flexion the inguinal ligament acts a flexor retinaculum as it supports the contents that are deep to the inguinal ligament. Therefore, this is can be considered an impingement site for nerves, arteries, veins, and lymph tissue at the hip deep to the inguinal ligament.
Femoral Pulse
The femoral pulse can be palpated when the individual is lying in a supine position. The femoral artery begins at the halfway point at the base of the femoral triangle just inferior to the inguinal ligament and midway between the anterior superior iliac spine (ASIS) and the pubic symphysis, known as the mid-inguinal point. The femoral pulse can be palpated by just inferior to the mid-inguinal point by pressing firmly. Normally the femoral pulse is strong, however, if the lumina (i.e., the inner cavity of a blood vessel) of the common or external iliac artery are partially occluded (i.e., blocked or obstructed), the pulse will reduce. Additionally, heavy bleeding in the lower extremity can be stopped by applying pressure at this point in the femoral triangle.
Angioplasties
The femoral triangle provides easy access to a major artery in the body (femoral artery) where coronary and peripheral angioplasties are often performed. Angioplasty is a procedure done to open a partially blocked blood vessel so that blood flow can flow through it more easily. The procedure includes the insertion of a thin flexible tube (catheter) through an artery in the groin (through the femoral triangle), arm (cubital fossa), or wrist and is carefully guided through the narrowed artery. Once the tube reaches the most narrow portion of the artery, a small balloon at the end of the tube (catheter) is inflated. This balloon will stay inflated for a short period of time and the pressure of the inflated balloon will press any fat or calcium deposits (i.e., plaque) against the walls of the artery to improve the flow of blood.
Femoral Hernia
By definition, a hernia is used to describe a bulge or protrusion of an organ through the structure or muscle that usually contains it (Medical Dictionary, 2018). The originating site for a femoral hernia is the femoral ring. A protrusion of the abdominal viscera (often a loop of the small intestine) through the femoral ring enters into the femoral canal. A femoral hernia appears as a lump or mass, which is often tender and appears in the femoral triangle just inferior to the inguinal ligament and lateral to adductor longus. Femoral hernias occur during an increase in pressure in the abdominal wall, for example, coughing, straining, heavy lifting, or pregnancy. Therefore, hernias in the femoral region are more common among female. Furthermore, a strangulation of a femoral hernia may occur due to the sharp, rigid boundaries of the femoral ring, more specifically the medial margin of the lacunar ligament (see figure 3). A strangulation of a femoral hernia simply means that the intestinal tissue that is projecting into the femoral ring is being cut off from its blood supply and this vascular impairment and can result in the death of the tissues. To release the strangulated hernia the lacunar ligament is cut, however, this procedure puts the aberrant artery that passes medially to the herniated sac at risk to be injured.
The Popliteal Fossa
Introduction & Borders
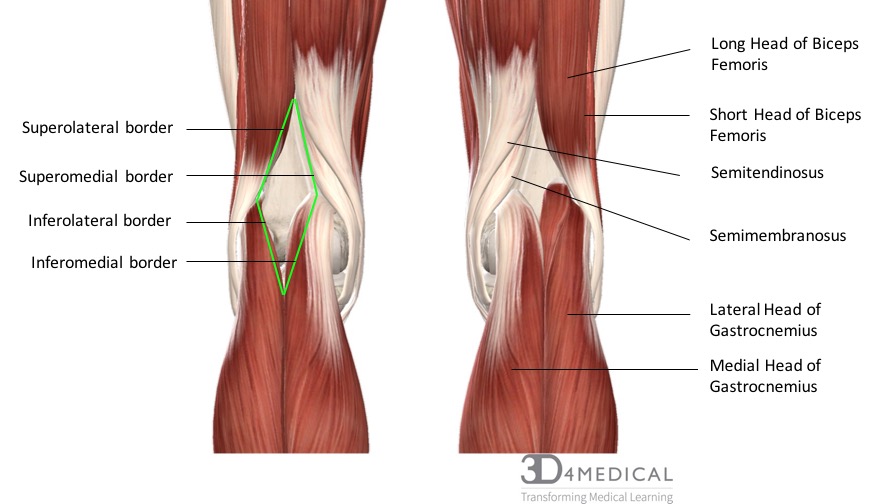
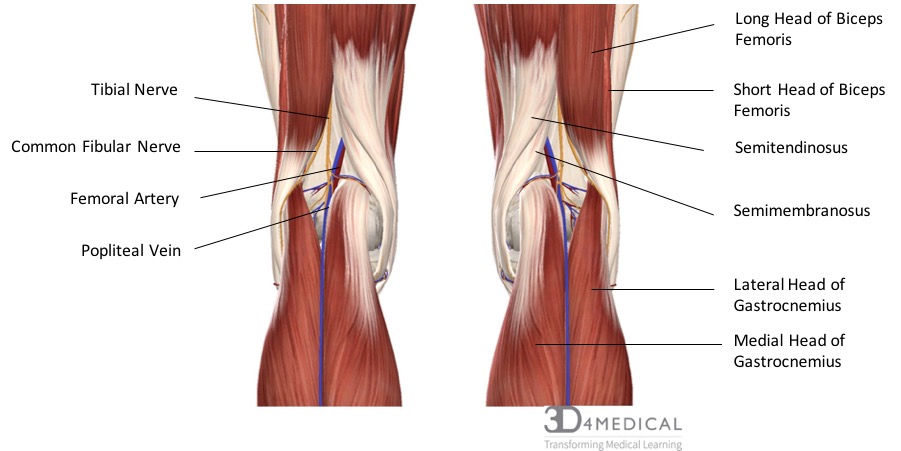
The popliteal fossa, sometimes called the knee pit, is a diamond-shaped area of vulnerability in the lower leg. It is located on the posterior side of the knee and is the main pathway for important structures moving from the thigh into the leg. There are four major muscles in the posterior compartment of the leg that forms the borders of the popliteal fossa. These include semimembranosus which forms the superomedial border, biceps femoris which forms the superolateral border, the medial head of gastrocnemius which forms the inferomedial border, and lastly the lateral head of gastrocnemius which forms the inferolateral border. Along with the muscles that form the borders the popliteal fossa also has a floor and a roof. The floor is formed by the posterior joint capsule in the knee and the posterior surface of the femur, while the roof is made up of popliteal fascia and skin.
Borders:
- Semimembranosus
- Biceps Femoris
- Gastrocnemius (medial head)
- Gastrocnemius (lateral Head)
Floor:
- Posterior Joint Capsule
- Posterior Surface of Femur
Roof:
- Popliteal Fascia
- Skin
Nervous Supply
Traveling through the popliteal are some of the major nerves, arteries, veins, and lymph that run through the posterior side of the leg. The two major nerves include the tibial nerve and the common fibular nerve. The tibial nerve arises from the sciatic nerve which splits just superior to the knee. The tibial nerve splits into an articular branch which works along with the obturator nerve for sensation to the knee, and a muscular branch which supplies all the muscles in the posterior compartment of the leg including gastrocnemius, soleus, plantaris, popliteus, tibialis posterior, flexor digitorum longus, and flexor halluces longus. The common fibular nerve, also called the peroneal nerve, arises from the lateral aspect of the sciatic nerve. It runs along the lateral condyle of the femur and then passes under fibularis longus where it then branches into the superficial fibular nerve and the deep fibular nerve. The common fibular nerve supplies the short head of biceps femoris in the thigh and its terminal branches supply all the muscles in the anterior and lateral compartments of the leg.
Arterial Supply
The main artery traveling through the popliteal fossa is the femoral artery which turns into the popliteal artery when it passes over the tibiofemoral joint. The femoral artery passes through the adductor hiatus in adductor magnus before entering the popliteal fossa and turning into the popliteal artery. The popliteal artery is the primary distributor of oxygenated blood to regions around the knee. Within the popliteal fossa the popliteal artery branches into other significant blood vessels such as the sural artery and the various types of genicular arteries. At the very distal end, the popliteal artery splits into the anterior and posterior tibial arteries which supply oxygenated blood to the lower leg.
Venous Supply
Running parallel to the popliteal artery is the popliteal vein which is formed from the anterior and posterior tibial veins. The popliteal vein is responsible for returning blood from the calf, the knee, and the thigh back to the heart. The small saphenous vein which originates in the foot empties into the popliteal vein as well as many of the genicular veins and the sural vein which surround the knee.
Lymphatic Supply
Within the popliteal fossa, there is many different lymph nodes and ducts. The main nodes in this region include the deep and superficial popliteal lymph nodes which are supplied by the medial superficial lymph vessels of the leg. These superficial lymph vessels lie within the superficial fascia of the leg and can be divided into a lateral and medial group. Both the deep and superficial lymph nodes and their vessels work together to drain the lower leg of lymph.
