Pelvis
Clinical Conditions
CLINICAL CONDITIONS OF THE PELVIC GIRDLE
Pubic Symphysis Dysfunction
Definition:
Pubic symphysis dysfunction (PSD) is a condition in which an excessive amount of movement occurs at the pubic symphysis of the pelvic girdle. Movement can come in anterior and lateral displacement.
Symptoms:
The main symptoms that are associated with PSD is usually pain or discomfort throughout the pelvic region, but usually centred on the pubic symphysis joint. Pain may also radiate to the back, abdomen and down through the thighs. In some cases, individuals who are suffering from PSD may feel and/or hear a clicking or popping while walking or when changing positions that cause movement of the pelvis. Associated pain arises because of possible alignment issues throughout the pelvis.
Causes:
PSD is most prevalent in women and is commonly associated with pregnancy and childbirth. During pregnancy, a hormone called relaxin is released to soften and loosen the ligaments and musculature of the pelvic floor and pelvic region. This release of relaxin, combined with increased weight load, ligament laxity and weakened musculature often manifests itself as PSD. Anatomical and genetic variations can also be a cause of PSD. In addition, contact sports such as rugby, American football, heavy weightlifting and extreme sports may compromise the stability of the pubic symphysis.
Treatment & Surgical Interventions:
If PSD is diagnosed during pregnancy, women are recommended to give birth in an upright position with knees parted slightly. A ribbon around the knees or legs is recommended to prevent the gap from exceeding maximal comfort zone. Postpartum, stabilizing and strengthening exercises are recommended to reduce pain associated with PSD. Pelvic support belts or lumbopelvic stabilizing belts may reduce symptoms of PSD. In severe cases, a wheelchair or surgery may be necessary to aid in the treatment of PSD.
Sacroiliitis
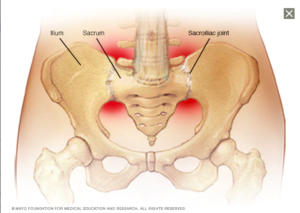
Figure 1. A visualization of the location of pain for sacroilitis. (Image retrieved from: https://www.mayoclinic.org/diseases-conditions/sacroiliitis/symptoms-causes/syc-20350747).
Definition:
Sacroiliitis (say-kroe-il-e-I-tis) is an inflammation of one or both of the sacroiliac joints (SI) of the pelvis. The sacroiliac joints are where the lower vertebrae attach to the pelvis, between the sacrum and ilia.
Symptoms:
Symptoms of sacroiliitis include pain in the lower back, hips, buttocks or thighs. Pain or stiffness may be exasperated by prolonged sitting or rolling out of bed. Occasionally, fever is associated with sacroiliitis.
Causes:
Because sacroiliits can be a description for any form of inflammation found with the SI joints, there can be a number of issues that can be the cause. Degenerative arthritis, or ostoarthritis can cause a degeneration of the bone within the SI joint, which then leads to the inflammation of the joint. Pregnancy can also cause inflammation of the joint from the widening and spreading of the pelvis in preparation for childbirth. Along with the widening, additional weight associated with childbearing can cause extra stress on the SI joint and lead to wear and inflammation. Traumatic injury from falls, car crashes or anything that has a direct affect on the low back, hips, buttocks or legs can also be a cause of sacroiliitis.
Treatment & Surgical Intervention:
Non-surgical treatments for sacroiliitis include rest, heat or ice and/or anti-inflammatory medications. Exercises aimed at stretching and strengthening the pelvic region have been shown to improve sacroiliitis symptoms. If pain persists, sacroiliac injections of a numbing agent and anti-inflammatory medication may be necessary. In extreme cases where non-surgical options failed, surgery may be necessary to fuse the sacroiliac joints and provide stability.
CLINICAL CONDITIONS OF THE HIP JOINT
Avascular Necrosis
Definition:
Avascular necrosis (AVN), is a condition in which there is a significant amount of blood loss to the area surrounding the head of the femur and results in the death of bone tissue. This condition can lead to a deterioration of the head of the femur, collapsed bone, and subsequent loss of joint congruity.
Symptoms:
In early stages, AVN is asymptomatic in the majority of patients. As AVN progresses, patients may experience pain only while weight-bearing and may eventually experience pain while in a supine position. Pain usually emerges gradually and can be mild to severe. Pain is usually experienced in the hip area but may affect the groin, buttocks or thigh.
Causes:
AVN is caused by an interruption or reduction of blood flow to bony tissue. This may be caused by dislocation, cancer treatment, fatty deposits in the blood or certain diseases, such as Gaucher’s disease or sickle cell anemia. Excessive alcohol intake and high-dose steroid medication use are also associated with AVN. In approximately 25% of patients, the cause of AVN is unknown.
Treatment & Surgical Intervention:
If caught in it’s early stages, AVN may be treated with nonsteroidal anti-inflammatories, osteoporosis medications, cholesterol lowering medications or blood thinners. Electrical stimulation, exercise and/or rest may also be prescribed. Unfortunately, because the early stages of AVN are generally asymptomatic, surgery may be recommended once diagnosed. Physicians may recommend core decompression, bone graft, bone reshaping, joint replacement or regenerative medicine treatment.
Hip Dysplasia
Definition:
Hip Dysplasia is a congenital condition that effects the acetabulum of the pelvis. With this condition, there is a loss of coverage of the head of the femur from the acetabulum and to compensate the body forms extra labrum tissue to help keep the head of the femur in place. As a result of this, the labrum because more active and overloaded and has shown a predisposition to tearing.
There are two forms of hip dysplasia:
Anterior acetabular dysplasia, refers to the anterior wall of the acetabulum where there is a lack of coverage at the front of the head of the femur.
Lateral acetabulur dysplasia, refers to the lack of ceovera of the lateral portion of the head of the femur, and the are on the side of the pelvis.
Symptoms:
Symptoms of hip dysplasia include partial or complete dislocation of the hip joint. In infancy, one leg may appear to be longer or one hip may be less flexible than the other. Once the infant starts walking, hip dysplasia may present as a limp. In teens and young adults, hip dysplasia may cause activity-related groin pain or a sensation of hip instability.
Causes:
Hip dysplasia is congenital and is caused by a shallow acetabulum (or socket) that does not form all around the head of the femur.
Treatment & Surgical Interventions:
During early infancy, a soft brace is generally utilized to correct the dysplasia and allow the socket to form the the shape of the head of the femur. After approximately 6 months of age, a soft brace is no longer effective and the physician may align the bones in the correct position and maintain that alignment with a full body cast for several months. If the hip dysplasia is severe, surgery or a periacetabular osteotomy may be required to reposition the socket at the appropriate position. In older adults, hip dysplasia can severely damage the hips, resulting in debilitating arthritis and hip replacement surgery can become necessary.
CLINICAL CONDITIONS OF THE GLUTEAL REGION
Superior Gluteal Nerve Injury
Definition:
Injury or damage to the superior gluteal nerve results in impaired function of the major hip abductor musculature: the gluteus medius and gluteus minimus muscles.
Symptoms:
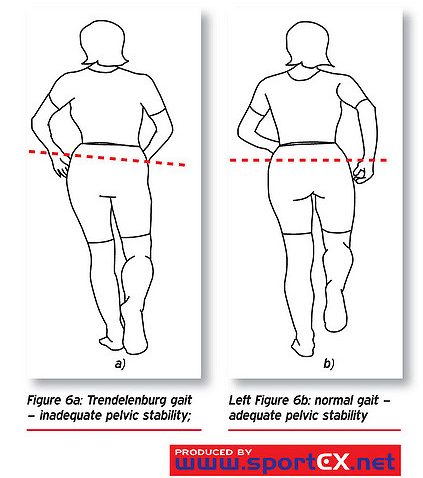
Under normal conditions the role of the gluteus medius and gluteus minimus muscles actively function during single-stance movement (as in walking) to prevent excessive dipping of the pelvis on the opposite and unsupported side. When the superior gluteal nerve is damaged, a unique gait occurs termed Trendelenburg’s Gait, in which the pelvis dips inferiorly opposite to the side of the site of injury.
This effectively lengthens the unsupported lower limb and makes clearing the ground during the swing phase of movement difficult. The person compensates for the abnormally lengthened position of the lower limb, by excessively leaning the trunk away from the unsupported side in an effort to shorten the limb and permit forward swing. Other compensation mechanisms include steppage gait, in which the foot lifts higher during the forward swing phase, and swing-out gait in which the foot digresses laterally or outward in an attempt to clear the ground during the swing phase.
Causes:
Injury or damage to the superior gluteal nerve are the most common causes. Nerve entrapment may also affect superior gluteal nerve function.
Treatment:
There are nerve flossing exercises that can help with superior gluteal nerve syndrome.
Piriformis Syndrome
Definition:
Piriformis syndrome can be divided into primary and secondary piriformis syndrome.
Symptoms:
Sciatic nerve compression symptomology can vary from mild irritation and discomfort, to debilitating pain that radiates the course of the sciatic nerve path from the gluteal region, posterior thigh, leg and to the lateral foot.
Causes:
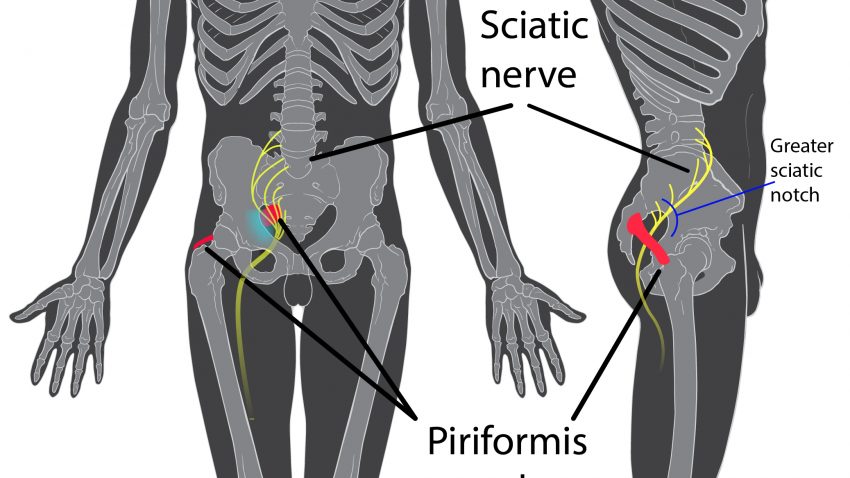
In primary piriformis syndrome, the musculoskeletal pain is caused by an anatomical variation in the path of the sciatic nerve relative to the piriformis. Normally, the sciatic nerve exits inferiorly to the piriformis via the infrapiriform foramen of the greater sciatic notch. However, in approximately 12% of the population the sciatic nerve bifurcates into the common fibular division before completely exiting the greater sciatic foramen and intersects the fibers of the piriformis muscle. In 0.5% of the population the common fibular division exits superiorly to the piriformis.
Secondary piriformis syndrome accounts for 50% of piriformis syndrome cases and arises due a specific injury to the buttocks, which can be micro-traumatic in nature such sitting repeatedly on hard surfaces, or macro-traumatic in nature such as a direct fall to the buttocks. Secondary piriformis syndrome accounts for 50% of piriformis syndrome cases. Inflammation and muscle spasms of the piriformis cause compression and irritation to the sciatic nerve that passes through the infrapiriform foramen. Other mechanisms of injury range from post-surgical injury, pathologies of the sacroiliac joint and lumbar spine, and overuse of the lateral rotators that cause hypertrophy of the piriformis and a resultant narrowing of the infrapiriform foramen that compress the sciatic nerve that exits through it.
Treatment:
Common treatment for piriformis syndrome is ice and heat therapy. Anti-inflammatory medications may aid in reducing piriformis syndrome pain. If pain and spasms are persistent, piriformis injections may be used. In extremely rare cases, the piriformis muscle has been surgically cut to relieve symptoms.
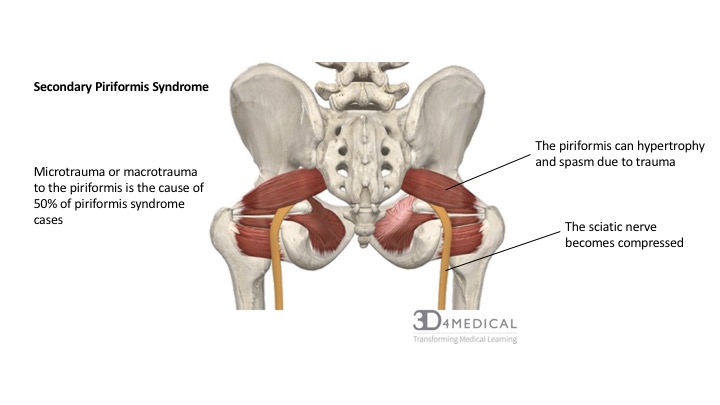
Figure 3. Visualization of piriformis syndrome.
Inferior Gluteal Nerve Injury
Definition:
The inferior gluteal nerve innervates the major extensor of the hip, the gluteus maximus muscle. Damage or entrapment of the inferior gluteal nerve is known as inferior gluteal nerve injury (IGNI). IGNI is often misdiagnosed as myofascial pain.
Symptoms:
Damage to this nerve results in a gluteus maximus atrophy and a gait abnormality called gluteus maximus lurch, which is characterized by a backward trunk lean upon heel strike on the affected side. This posterior hinge of the trunk is a compensatory hip extension mechanism. Normally, the gluteus maximus briefly contracts upon heel strike to decelerate forward motion of the trunk via initiating hip extension. Without activation of the gluteus maximus the trunk hyperextends in an effort to maintain balance during the stance phase, and often the hamstring muscles compensate as the primary hip extensors in an attempt to normalize the gait.
Causes:
While injury to this nerve is less common that that of the superior gluteal nerve, it is commonly associated with damage during hip replacement surgery. Iatrogenic injury is the most common cause of injury to the gluteal nerves.
Treatment:
Common treatment for IGNI consists of nerve flossing exercises.
PELVIC FLOOR
Normal pelvic floor muscles can contract involuntarily and voluntarily with normal strength and ability to relax completely. Non-contracting pelvic floor muscles (underactive) cannot voluntarily contract. Non-relaxing (overactive) pelvic floor muscles do not relax and might contract when relaxation is need such as during defecation or urination. Nonfunctioning pelvic floor muscles do not response to palpation and can be both weak and hypertonic being a mix of non-contracting and non-relaxing.
Incontinence (urinary)
Definition:
The pelvic floor provides support through constant muscular contraction with passive support from surrounding connective tissues. An increase in intraabdominal pressure triggers a reflexive contraction in an upward motion of the pelvic floor and closure of vagina, urethral, and anal sphincters. If this action does not occur correctly then incontinence can occur.
Symptoms:
Urinary incontinence is characterized by the inability to control the bladder. Urinary incontinence occurs when the bladder neck cannot be held closed, leading to a leak in urine.
Causes:
Urinary tract infections may be a cause of temporary urinary incontinence. Urinary incontinence is also commonly caused by pelvic floor dysfunction. Weak muscles of the pelvic floor affect the sphincteric function. Pregnancy, childbirth, increase in age, obstruction of the urinary tract and neurological disorders can also affect urinary incontinence.
Treatment:
Treatment for urinary incontinence include behavioural techniques, pelvic floor exercises, electrical stimulation, medications, medical devices, absorbent pads and catheters. Behavioural techniques include things such as bladder training, scheduled bathroom trips and fluid management. Medical devices include urethral inserts or pessary. In extreme cases, surgery may be required to treat the causes of urinary incontinence.
Incontinence (anal)
Definition:
Defecation or a bowel movement occurs when the anal sphincter and puborectalis muscles relax opening rectoanal angle and allowing the feces to pass. This relaxation is reflexive through the autonomic nervous system. Concurrent with relaxation an increase in abdominal pressure occurs during the contraction of the abdominal muscles during a Valsalva maneuver. If the anal sphincter and puborectalis muscles do not stay contracted incontinence can occur.
Symptoms:
Rectal incontinence is characterized by the inability to control the anal sphincter. Rectal incontinence occurs when the anal sphincter is not contracted and defecation or a bowel movement occurs.
Causes:
Rectal incontinence can be caused by diarrhea, constipation, muscle injury or weakness, hemorrhoids, rectal prolapse, childbirth, physical inactivity, or rectocele. Nerve damage or neurological diseases may also affect rectal incontinence.
Treatment:
Treatment for rectal incontinence can include absorbent pads, diet changes, bowel training, pelvic floor exercises and medications. Physicians may utilize feedback therapy, sacral nerve stimulation, vaginal balloons and non-absorbable bulking agents. In extreme cases, surgery may be necessary to treat rectal incontinence.
Pelvic organ prolapse
Definition:
Pelvic organ prolapse is a hernia of the pelvic organs through the urogenital hiatus. It is more common in women than men due to the larger urogenital hiatus that the urethra and vagina pass through. Pelvic organs can drop lower in the pelvis resulting in a bulge in the vagina (prolapse).
Symptoms:
Symptoms of pelvic organ prolapse can include a feeling of fullness in the pelvis, low back pain, painful sexual intercourse, or the feeling that something is going to fall out of the vagina.
Causes:
Prolapse can occur due to trauma to the pelvic floor or due to poor tone to the muscle fibres. Prolapse is also common with damage to the perineal body during childbirth. Prolapse can be broken down into two types, symptomatic and asymptomatic. Symptomatic refers to when tissue protrudes past the vaginal opening. Asymptomatic refers to when the hernia has taken place but no tissue extends past the vaginal opening.
Treatment:
In the case of mild, asymptomatic pelvic organ prolapse, common treatment is time, as pelvic organ prolapses are known to improve on their own. Pessaries and behavioural treatment may also be utilized to treat pelvic organ prolapse. In extreme cases, pelvic reconstruction or surgery may be used as a treatment, however there is approximately 30% chance of reoccurrence.
GYNAECOLOGICAL CLINICAL CONDITIONS
Pelvic Inflammatory Disease
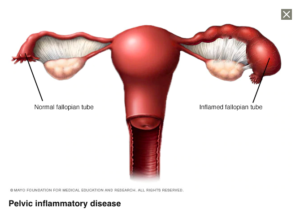
Figure 5. A visualization of PID. (Image retrieved from:https://www.mayoclinic.org/diseases-conditions/pelvic-inflammatory-disease/symptoms-causes/syc-20352594).
Definition:
Pelvic inflammatory disease (PID) is an inflammation or infection of the female upper genital tract, including the fallopian tubes, ovaries and womb. PID most commonly affects sexually active women aged 15-24.
Symptoms:
Symptoms can include pain in the pelvic or lower abdominal region, painful or heavy menstruation, pain during urination, bleeding between menstruation or following sexual intercourse, discomfort or pain deep in the pelvis during sexual intercourse and unusual vaginal discharge.
Causes:
PID is caused by a bacterial infection that spreads from the cervix or vagina to the superior reproductive organs. In approximately 1 out of 4 cases, PID is caused from a sexually transmitted infection (STI) like gonorrhoea or chlamydia. Mycoplasma genitalium is another STI thought to be increasingly responsible for PID.
Treatment:
Treatment of PID is a course of antibiotics, usually by injection and tablet.
Endometriosis
Definition:
Endometriosis (en-doh-mee-tree-OH-sus) is a condition where the endometrium (lining of the uterus) grows outside the uterus. The endometrium can attach to fallopian tubes, ovaries, intestines and other structures in the pelvis.
Symptoms:
While endometriosis is a common clinical condition, it may be asymptomatic. However, endometriosis can also cause pelvic pain, especially during menstruation. Hormones released during the menstrual cycle cause the endometrium to bleed each month, which can be painful and lead to the formation of pelvic adhesions, or scar tissue. If blood builds up in the ovaries, it can result in a cyst and is referred to as endometrioma. Endometriosis has also been known to cause issues with fertility.
Causes:
The cause of endometriosis is endometrium growing outside of the uterus. Adenomyosis is a condition that occurs when the endometrium grows into the uterine muscles.
Treatment:
Anti-inflammatory medications may be used to treat endometriosis. Hormone therapy is another common treatment. Laparoscopic surgery to remove implants and adhesions may be necessary, and in extreme cases, a hysterectomy may be required to remove the uterus and ovaries.
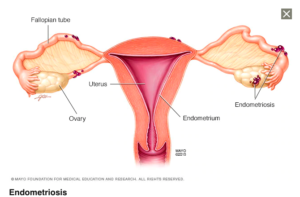
Figure 6. A visualization of endometriosis. (Image retrieved from: https://www.mayoclinic.org/diseases-conditions/endometriosis/symptoms-causes/syc-20354656).
Pelvic Adhesions
Definition:
Adhesions are scar tissue bands that can bind internal organs together. Infection, surgery or endometriosis can cause adhesions to form.
Symptoms:
Symptoms of pelvic adhesions include localized pain or generalized discomfort in the pelvic region.
Causes:
Pelvic adhesions can result from previous infections, pelvic and abdominal surgery, or endometriosis. Diagnosing adhesions can be difficult and a definitive diagnosis usually occurs during surgical exploration, most frequently via laparoscopy. In some cases, adhesions can cause the ovaries and uterus to feel bound together during pelvic examination.
Treatment:
Cutting bands of scar tissue via surgery can relieve pain, however adhesions have been known to re-form.
Vulvodynia
Definition:
Pain at the vaginal opening or surrounding lips (vulva) is referred to as vulvodynia.
Symptoms:
Symptoms can include irritation, burning, stinging, rawness or stabbing. The pain may be localized or diffused, intermittent or constant. Women with vulvodynia may experience pain during sexual intercourse, while inserting a tampon or while wearing tight fitting pants.
Causes:
While the cause of vulvodynia is unknown, it is thought to result from inflamed tissues, nerves and muscles in the pelvic area.
Treatment:
Treatment for vulvodynia can include lukewarm or sitz baths, ice or heat therapies, or relaxation techniques.
Pelvic Congestion Syndrome
Definition:
Pelvic congestion syndrome occurs when blood pools within the veins of the pelvic region.
Symptoms:
Symptoms of pelvic congestion syndrome include chronic pelvic pain, the feeling of needing the urinate and enlarged veins of the pelvic region and thighs.
Causes:
The causes of pelvic congestion syndrome are unclear but theories include enlarged veins in the pelvis and hormone production. Estrogen and other hormones dilate veins and may play a role in pelvic congestion syndrome.
Treatment:
Treatment may include medications such as progestin or gonadotrophin-releasing drugs to relieve pain. Embolization may be used to shut off veins and surgery may be required to remove damaged veins, the uterus or ovaries.
