Upper Limb
Special Anatomical Regions
THE AXILLA
– The axilla provides a passageway, or ‘distribution center’, for vessels and nerves to reach the upper limb. It is located inferior to the glenohumeral joint and superior to the axillary fascia at the junction of the arm and thorax
Visualizing the axilla and its contents
– The axillary inlet, outlet, and walls of the axilla can be established using skin folds and palpable bony landmarks. Major blood vessels, nerves, and lymphatics travel between the upper limb to the trunk through the axilla. For example, the axillary artery passes just inferior to the tip of the coracoid process and courses posterior to the coracobrachialis. Then the axillary artery, axillary vein, and components of the brachial plexus pass through the axilla by traveling laterally to the dome of skin that forms the floor. The neurovascular bundle can be palpated by placing a hand into this dome of skin and pressing laterally against the humerus.
Axillary inlet: The anterior margin is the clavicle and the lateral limit is approximately the coracoid process.
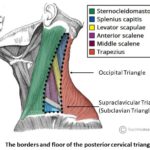
Axillary walls: The inferior margin of the anterior wall is the anterior axillary fold and the inferior margin of the posterior wall is the posterior axillary fold. The medial wall is the upper part of the serratus anterior muscle overlying the thoracic wall. The lateral wall is the humerus.
Axillary outlet: The floor of the axilla is the dome of skin between the posterior and anterior axillary folds.
– The axilla region is at its most vulnerable when the arm is fully abducted, a tickle reflex causes most people to rapidly adduct the arm allow for full protection of the area.
Introduction: (general boundaries)
Apex, base and 4 walls (anterior, medial, lateral, posterior)
*ref to pec/upper arm for muscles
@ Apex/ inlet: the apex of the axilla is surrounded by the:
– Clavicle (ant.)
– Scapula (post.)
– First rib (med.)
– Also known as a cervicoaxillary canal (NAVEL pass through to reach the arm)
@ Base/ skin: the base of the axilla is formed by the:
– Also known as the axillary fossa (armpit)
– Concave skin and fascia that extends from the arm to the chest wall
– Contains hair and deep to the base the lymph nodes can be palpated
@ Anterior wall: anterior wall of the axilla is composed mainly of the:
– Pec major
– Subclavis
– Clavipectoral fascia (anterior axillary fold, can be pinched between the fingers)
@ Posterior wall: posterior wall of the axilla is formed mainly by the:
– Subscapularis
– Teres major
– Latissimus dorsi
– Long head triceps brachii
– Posterior axillary fold, formed by the tendons of the lat and teres major (z)
@ Medial wall:
– Ribs 1-4 (upper thoracic wall)
– Intercostal muscles
– Serratus anterior
@ Lateral wall:
– Coracobrachialis
– Biceps brachii muscles
– Superior portion of the shaft of the humerus (intertubercular grove
*For details on musculature, refer to UPPER LIMB MUSCLES


NERVOUS, BLOOD VESSELS and LYMPH
Contents of the AXILLA via NAVEL (Nerves, Arteries, Veins, (Empty), Lymph)
N:
Brachial Plexus
The brachial plexus is divided into supraclavicular and infraclavicular parts by the clavicle. 4 branches of the supraclavicular arise from the roots and trunks of the brachial plexus (the dorsal scapular nerve, the long thoracic, nerve to subclavius and suprascapular nerve) and are approachable through the neck. Branches of the infraclavicular part of the plexus arise from the cords of brachial plexus and are approachable through the axilla (see Table 1 for the list of structures innervated).
Most nerves in the upper limb arise from the brachial plexus a major nerve network supplying the upper limb; it begins at the neck and extends into and through the axilla. Almost all branches of the brachial plexus arise in the axilla after it has crossed the 1st rib. The brachial plexus starts at the roots of 4 cervical and 1 thoracic nerve (C5-T1). The roots pass through the gap between the anterior and middle scalene muscles. In the inferior part of the neck, the roots of the brachial plexus unite to form 3 trunks:
- Superior trunk, union of C5 and C6 roots
- Middle trunk, a continuation of C7
- Inferior trunk, union of C8 and T1
Each trunk of the brachial plexus divides into anterior and posterior divisions as the plexus passes through the cervicoaxillary canal (aka the apex of the axilla) posterior to the clavicle. Anterior divisions of the trunks supply anterior or flexor compartments of the upper limb, and the posterior divisions of the trunks supply posterior or extensor compartments of the upper limb. The divisions of the trunks form 3 cords:
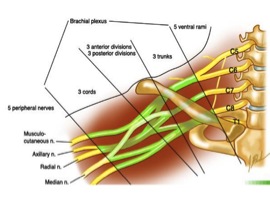
- Anterior divisions of the superior and middle trunks unite to form the lateral cord
- Anterior division of the inferior trunk continues as medial cord
- Posterior divisions of all 3 trunks unite to form the posterior cord
The cords follow or pair with the axillary artery, for example, the lateral cord is lateral to the axillary artery.
The peripheral nerves branch from the cords to form the terminal branches, 3 branches arise from the lateral cord, 5 branches from medial and posterior cords
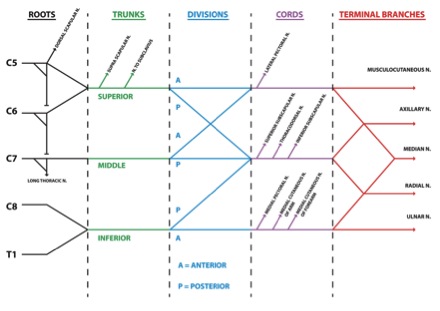
Table 1: Brachial Plexus and Nerves of Upper Limb
| NERVE | ORIGIN | COURSE | STRUCTURES INNERVATED |
| *Supraclavicular branches | |||
| Dorsal Scapular | Posterior aspect of anterior of C5, contribution from C4 | Through middle scalene, descends deep to levator scapulae and rhomboids | Rhomboids: occasionally supplies levator scapulae |
| Long Thoracic | Posterior aspect of C5, C6, C4 | Passes through cervicoaxillary canal, descending posterior to C8 and T1 roots of plexus; runs inferiorly on superficial surface of serratus anterior | Serratus anterior |
| Suprascapular | Superior trunk, receiving fibers from C5, C6, C4 | Passes laterally across lateral cervical region (posterior triangle of neck), superior to brachial plexus; then through scapular notch inferior to superior transverse scapular ligament | Supraspinatus and infraspinatus muscles; glenohumeral joint (shoulder) |
| Subclavian Nerve | Superior trunk, receiving fibers from C5, C6, C4 | Descends posteriorly to clavicle and anterior to brachial plexus and subclavian artery; often giving an accessory root to phrenic nerve | Subclavius and sternoclavicular joint (accessory phrenic root innervates diaphragm) |
| * Infraclavicular branches | |||
| Lateral Pectoral | Side branch of lateral cord receiving fibers from C5, C6, C7 | Pierces costocoracoid membrane to reach deep surface of pectoral muscle; a communicating branch to the medial pectoral nerve passes anterior to axillary artery and vein | Primarily pectoralis major; but some lateral pectoral nerve fibers pass to pectoralis minor via branch to medial pectoral nerve |
| Musculocutaneous | Terminal branch of lateral cord, receiving fibers from C5-C7 | Exits axilla by piercing coracobrachialis; decends between biceps brachii and brachialis, supplying both | Muscles of anterior compartment of arm (coracobrachalis, biceps brachaii and brachilias), skin of lateral aspect of forearm |
| Median | Lateral root of median nerve is a terminal branch of lateral cord C6, C7
Medial root of median nerve is a terminal branch of medial cord C8, T1 |
Lateral and medial roots merge to form median nerve lateral to axillary artery; descends through arm adjacent to brachial artery, with gradually crossing anterior to artery to lie medial to artery in cubital fossa | Muscles of anterior compartment (except flexor carpi ulnaris and ulnar half of flexor digitorum profundus), five extrinsic muscles in thenar half of palm and palmar skin |
| Ulnar | Larger terminal branch of medial cord, receiving fibers from C8, T1, C7 | Descends medial arm; passes posterior to medial epicondyle of humerus; then descends ulnar aspect of forearm to hand | Flexor carpi ulnaris and ulnar half of flexor digitorium profundus; most intrinsic muscles of the hand |
| Upper subscapular | Side branch of posterior cord, receiving fibers from C5 | Passes posteriorly, entering subscapularis directly | Superior portion of subscapularis |
| Lower subscapular | Side branch of posterior cord, receiving fibers from C6 | Passes inferolaterally, deep to subscapular artery and vein | Inferior portion of subscapularis and teres major |
| Thoracodorsal | Side branch of posterior cord, receiving fibers from C6, C7, C8 | Arises between upper and lower subscapular nerves and runs inferolatterally along posterior axillary wall to apical part of latissimus dorsi | Latissimus dorsi |
| Axillary | Terminal branch of posterior cord, receiving fibers from C5, C6 | Exits axillary fossa posteriorly, passing through quadrangular space with posterior circumflex humeral artery; gives rise to superior lateral brachial cutaneous nerve; then winds around surgical neck of humerus deep to deltoid | Glenohumeral joint; teres minor and deltoid muscles |
| Radial | Larger terminal branch of posterior cord (largest branch of plexus), receiving fibers from C5- T1 | Exits axillary fossa posterior to axillary artery, passes posterior to humerus in radial groove with deep brachial artery, between lateral and medial heads of triceps; perforates lateral intramuscular septum; enters cubital fossa, dividing into superficial and deep radial nerves | All muscles of posterior compartments of arm and forearm |
A:
Axillary Artery
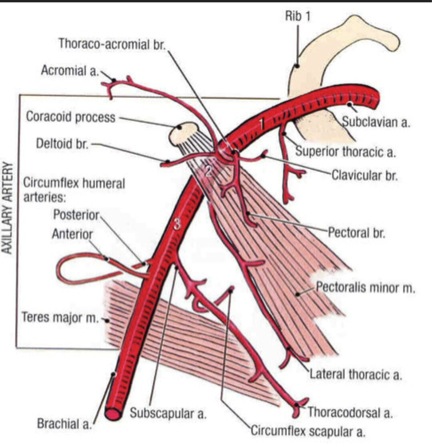
The axillary artery begins at the lateral border of the 1st rib as the continuation of the subclavian artery and ends at the inferior border of the teres major. It passes posterior to the pectoralis minor into the arm and becomes the brachial artery when it passes the inferior border of the teres major, at which point it has reached the humerus.
- The first part of axillary artery is located between the lateral border of the 1st rib and the medial border of the pectoralis minor; it is enclosed in an axillary sheath, it has one branch, the superior thoracic artery
- The second part of the axillary artery lies posterior to pectoralis minor and has 2 branches: thoracoacromial and lateral thoracic arteries
- The third part of the axillary artery extends from the lateral border of pectoralis minor to the inferior border of teres major and has 3 branches: subscapular, anterior circumflex humeral and posterior circumflex arteries
The axillary artery is a large muscular vessel that travels through the axilla. It is responsible for carrying oxygen-rich blood to the upper limb, as well as to parts of the musculocutaneous system of the scapula and upper lateral thorax.
The neurovascular bundle formed by the artery and the axillary fascia envelops the cords of the brachial plexus. The fascia is then attached to the suspensory ligaments of the axilla (a continuation of the clavipectoral fascia) for additional protection. As a result of this attachment, the axillary artery is more easily palpated in the concavity of the axilla when the upper arm is adducted (close to the midline of the body) and the suspensory ligaments are relaxed, than when it is abducted (away from the midline of the body) and the suspensory ligaments are taut.
Some interesting facts:
- Compression of axillary artery against humerus can stop bleeding
- Aneurysm of the axillary artery can compress the trunks of the brachial plexus and cause loss of skin sensation in the area
V:
Axillary Vein
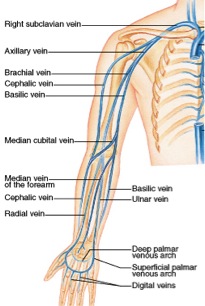
The axillary vein is a large blood vessel that conveys blood from the lateral aspect of the thorax, axilla (armpit) and upper limb toward the heart. There is one axillary vein on each side of the body. Its origin is at the lower margin of the tres major muscle and a continuation of the brachial vein. This large vein is formed by the brachial vein and the basilic vein at its terminal part; it is also joined by the cephalic vein. Other tributaries include the subscapular vein, circumflex humeral vein, lateral thoracic vein, and thoraco-acromial vein. It terminates at the lateral margin of the first rib, at which it becomes the subclavian vein. It is accompanied along its course by a similarly named artery, the axillary artery.
E:
Empty
L:
Axillary lymph
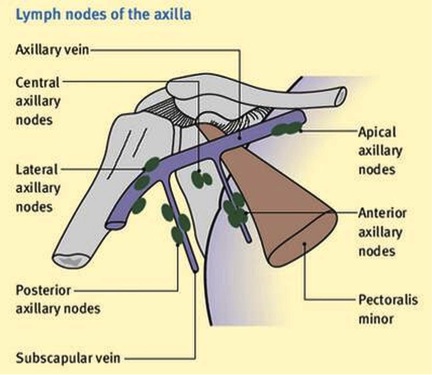
The axillary lymph nodes filter lymph that has drained from the upper limb and pectoral region. In women, axillary lymph node enlargement is a non-specific indicator of breast cancer. The body has about 20 to 40 bean-shaped axillary lymph nodes located in the underarm area. These lymph nodes are responsible for draining lymph – a clear or white fluid made up of white blood cells – from the breasts and surrounding areas, including the neck, the upper arms, and the underarm area. They are about 1cm in size and are arranged into five groups: subscapular axillary (posterior), apical (medial or subclavicular), pectoral axillary (anterior), brachial (lateral), and central lymph nodes. The subscapular axillary lymph nodes are located on the lower part of the armpit’s posterior (rear) wall. The apical and pectoral nodes are located respectively on the upper and lower parts of the pectoralis minor, a thin, flat muscle of the chest. The brachial nodes are located relative to the axillary vein’s medial (near the middle) and posterior portions. The central axillary lymph nodes are located inside the adipose tissue near the armpit’s base. Breast cancer initially develops as a lump in the breast, but often spreads to the axillary lymph nodes, which allows it to access the lymphatic system and travel to other areas of the body. During surgical procedures to remove breast cancer, including lumpectomies and partial, modified radical, radical, or total mastectomies, surgeons often remove some of the axillary lymph nodes to determine whether the breast cancer has spread, and also to determine cancer staging.
Clinical Significance of Axillary region
– Thoracic Outlet Syndrome
The apex of the axilla region is an opening between the clavicle, first rib, and the scapula. In this apex, the vessels and nerves may become compressed between the bones – this is called thoracic outlet syndrome. Common causes of TOS are trauma (fractured clavicle) and repetitive actions (seen commonly in occupations that require lifting of the arms). It often presents with pain in the affected limb, (where the pain is depends on what nerves are affected), tingling, muscle weakness, and discoloration.
– Compression of Axillary Artery
The axillary artery can be palpated in the inferior part of the lateral wall of the axilla. Compression of the third part of this artery against the humerus may be necessary when profuse bleeding occurs (resulting from a stab or bullet wound in the axilla). If compression is required at a more proximal site, the axillary artery can be compressed at its origin (as the subclavian artery crosses the 1st rib) by exerting downward pressure in the angle between the clavicle and the inferior attachment of the sternocleidomastoid.
– Aneurysm of Axillary Artery
The first part of the axillary artery may enlarge and compress the trunks of the brachial plexus, causing pain and anesthesia (loss of sensation) in the areas of the skin supplied by the affected nerves. Aneurysm of the axillary artery may occur in baseball pitchers because of their rapid and forceful arm movements.
– Brachial Plexus Injuries
Brachial plexus injuries vary greatly in severity, depending upon the type of injury and the amount of force placed on the plexus. The same patient can injure several different nerves of the brachial plexus in varying severity.
- Avulsion. In this most severe brachial plexus injury, the nerve root has been torn from the spinal cord. These types of injuries may not be repairable with surgery.
- Stretch (Neuropraxia). When the nerve is mildly stretched, it may heal on its own or require simple, nonsurgical treatment methods to return to normal function.
- Rupture. A more forceful stretch of the nerve may cause it to tear partially or fully. These types of injuries can sometimes be repaired with surgery.
More information can found at:
https://orthoinfo.aaos.org/en/diseases–conditions/brachial-plexus-injuries/
THE CUBITAL FOSSA
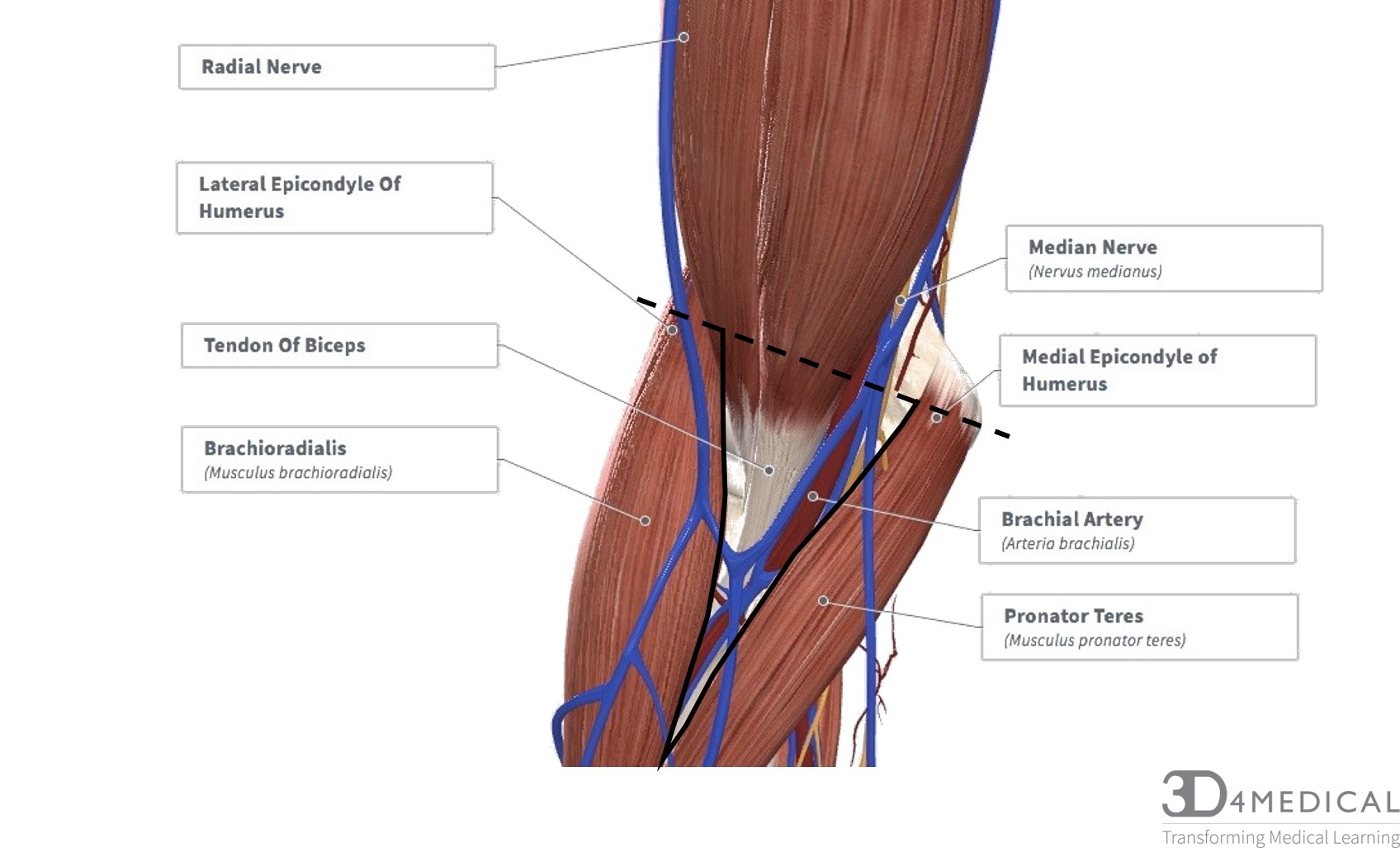
The cubital fossa or the antecubital fossa is located on the anti-brachium (forearm). This triangular space is the transition space from the arm to the forearm. The cubital fossa resembles the shape of a triangle containing three borders; The superior border, medial border, and the lateral border. The superior border is an imaginary line connecting the medial and lateral epicondyles. The lateral border being the muscle belly of brachioradialis, and the medial border being the muscle belly of pronator teres. Within the fossa runs numerous arteries, veins, and nerves. Because of the location and the contents running through and around this fossa, this makes for a very significant clinical area.
Boundaries
- Medial and lateral epicondyles (superior border)
- Brachioradialis (lateral border)
- Pronator Teres (medial border)
Floor
- Brachialis, Supinator
Roof
- Deep fascia of the forearm (Bicipital aponeurosis)
If we were to remove the muscles covering the cubital fossa, the contents listed below would be revealed, we will list these contents as they appear medial to lateral.
Main Contents
- Median Nerve
- Brachial Artery
- Tendon of Biceps
- Radial Nerve
Clinical Significance
Because of the fossa’s location and contents, this makes for a very clinically significant area.
Brachial pulse and Blood pressure: During blood pressure, the stethoscope is placed on the cubital fossa while the cuff is inflated around the humerus restring blood flow through the arm from the brachial artery.

Venipuncture: Like mentioned, there are numerous veins and arteries running through and over the fossa making it for a very accessible area for venipuncture. These can be used for drawing blood, inserting a catheter and also for intravenous feeding.

