Pelvis
Muscles
Muscles of the Pelvis
Gluteal Region
The musculature of the gluteal region can be divided into two distinct regions: a superficial layer consisting of four muscles responsible for hip abduction, extension, and medial rotation and a deep layer consisting of six muscles responsible for lateral rotation of the hip joint.
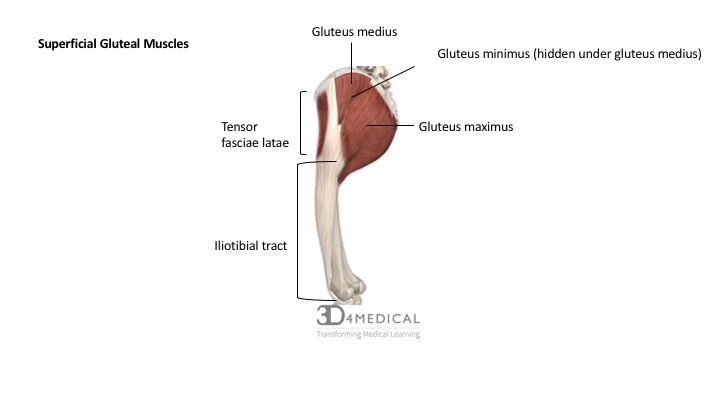
Figure 1. Diagram summarizing the muscles location of the gluteal group.
Gluteus Maximus
Structure
The gluteus maximus is the heaviest and largest muscle in the body according to its cross-sectional area, volume and thickness. According to studies, gluteus maximus is twice as heavy as the gluteus medius muscle and 27% heavier than the second heaviest muscle in the body, the adductor magnus.
The most superficial of the three gluteal muscles, the gluteus maximus forms the surface anatomy of the gluteal region overlapping the majority of the gluteus medius muscle and completely covering the deepest gluteal muscle, the gluteus minimus.
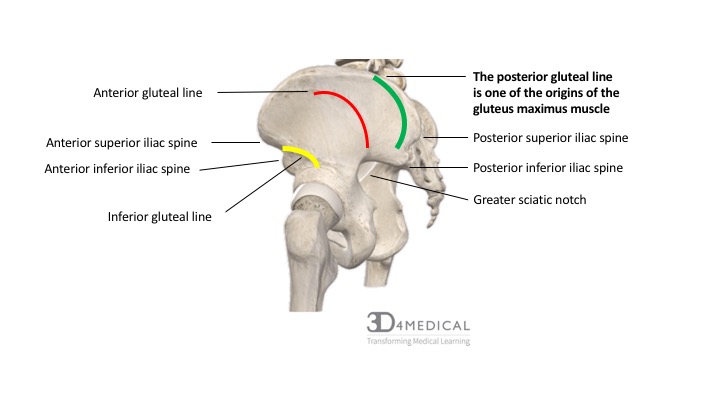
A heavily-pennated and densely-fibered muscle, the gluteus maximus is a complex muscle with a number of origins including the posterior gluteal line of the ilium, posterior surface of the sacrum, coccyx, aponeurosis of sacrospinalis ligament, the sacrotuberous ligament and the fascia covering the gluteus medius (gluteal aponeurosis). Approximately 75% of the gluteus maximus fibers insert into the iliotibial tract of the fascia latae, while 25% of the fibers insert into the gluteal tuberosity of the femur.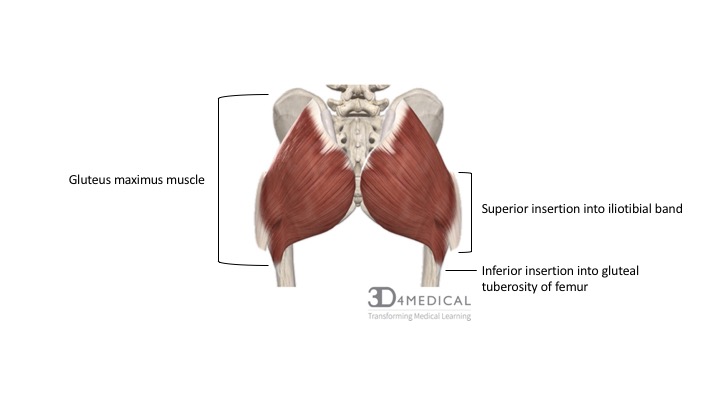
Figure 2. Diagram summarizing the insertion points of the gluteus maximus muscle.
Function
Given the wide range of origins, as well as a superior and inferior insertion, the gluteus maximus muscle performs a variety of actions including hip extension, lateral rotation (external rotation) and trunk extension when the distal attachment of the muscle is fixed. The superior fibers of the muscle also work through their connection with the iliotibial band to provide support to the knee during extension, while the inferior fibers of the gluteus maximus affect posterior tilt of the pelvis.
Although the gluteus maximus muscle is the strongest hip extensor and is predominantly activated during powerful or rapid force movements such as sprinting, stair climbing, or rising from a flexed to extended thigh positioning, it remains fairly inactive during walking and almost completely inactive during standing.
Innervation
The gluteus maximus is innervated by the inferior gluteal nerve (L5 – S2).
Gluteus Medius and Gluteus Minimus
Structure
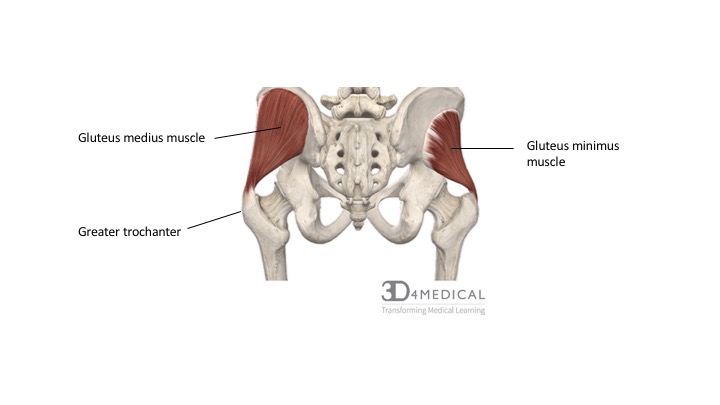
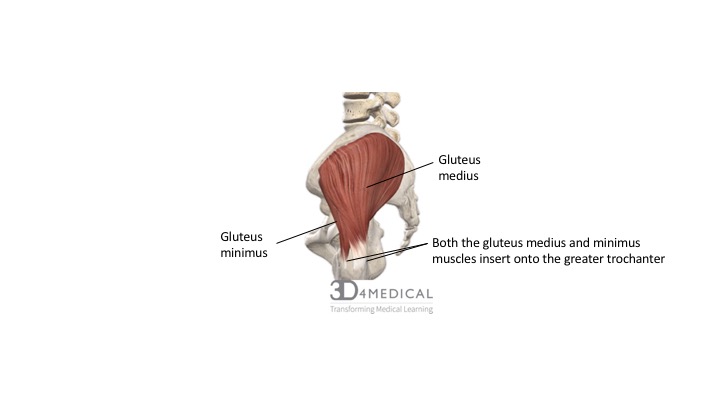
Comparably smaller and laying deep to the gluteus maximus muscle, the fan-shaped gluteus medius and gluteus minimus muscles both originate on the external surface of the ilium and have similar insertion points on the greater trochanter of the femur.
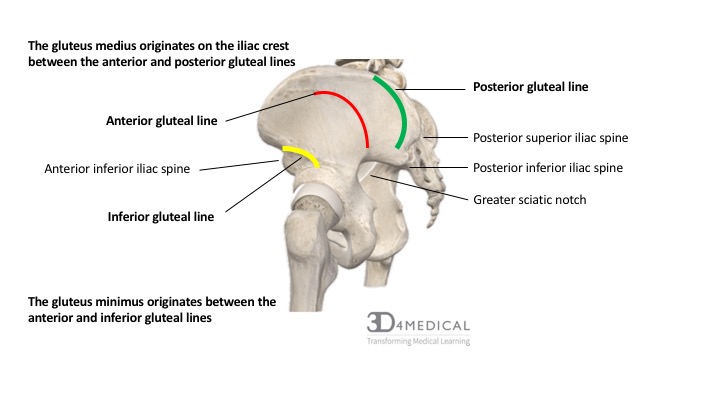
The gluteus medius muscle originates on the anterior gluteal surface of the ilium, between the iliac crest and posterior gluteal line above and the anterior gluteal line below (see photo below), the gluteal aponeurosis (thick fascia covering the gluteus medius) and inserts into the lateral surface of the greater trochanter of the femur.
The gluteus minimus muscle originates just inferior to the origin of the gluteus medius between the anterior and inferior gluteal surface of the ilium and inserts on the anterior surface of the greater trochanter of the femur.
Function
The primary actions of the gluteus medius and gluteus minimus are hip abduction and medial rotation. They also work to contribute to hip stability particularly during single-leg stance movements and to increase the congruency of the femoral head within the acetabulum.
Innervation
Both the gluteus medius and minimus are innervated by the superior gluteal nerve (L5 – S1).
Tensor Fasciae Latae
Structure
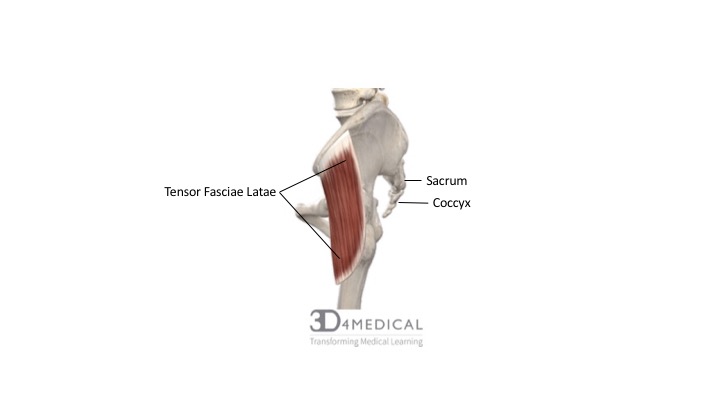
The tensor fasciae latae (TFL) is a fusiform (spindle-like) muscle, approximately 15 cm in length that originates at the anterior superior iliac spine and the anterior portion of the iliac crest. Sandwiched between two layers of fasciae latae, the TFL shares an insertion point along with the gluteus maximus muscle into the iliotibial tract. Despite this shared insertion with the gluteus maximus muscle, the TFL is conversely innervated by the superior gluteal nerve and acts in opposition to the gluteus maximus to provide hip flexion.
Function
Due to the anterior location on the ilium, the TFL works synergistically with the iliopsoas and rectus femoris to perform hip flexion, medial rotation of the hip and also tenses the iliotibial band to provide lateral knee stability.
Innervation
The tensor fasciae latae is innervated via the superior gluteal nerve (L5 – S1).
Iliotibial Band
Structure
The iliotibial band, also known as the IT band or Maissiat’s band, is a deep fascia that originates both from the continuation of the tensor fasciae latae, as well as from the superior insertion point of the gluteus maximus. While it is not considered as a muscle of the gluteal region, its included in the gluteal muscle group because its fibers merge with those of the gluteus maximus and are a continuation of the tensor fasciae latae.
The superior origin of the IT band is spliced into two layers that blend with both the TFL and the tendinous insertion of the gluteus maximus muscle. The IT band spans the lateral surface of the femur, crossing the knee joint and inserting onto the lateral tibial plateau of the tibia.
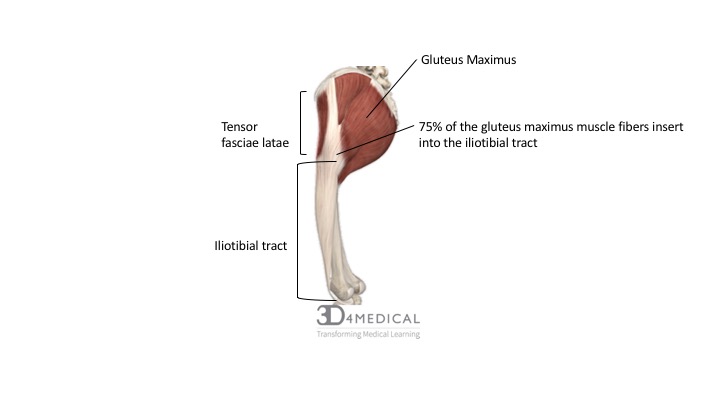
Figure 8. Diagram demonstrating the sagittal view of the tensor fascia latae origin and insertion points.
Function
Based on its lengthy span from the tensor fasciae latae to its insertion at the lateral epicondyle of the tibia, the iliotibial band functions as an abductor, medial rotator and flexor of the thigh. Collectively, the tensor fasciae latae, gluteus maximus work through the iliotibial band to stabilize the knee during extension phases of standing, walking, running and biking.
Innervation
The iliotibial band is innervated by the inferior gluteal nerve (L5 – S2).
| SUPERFICIAL MUSCLES OF THE GLUTEAL REGION | ||||
| Muscle | Origin | Insertion | Innervation | Action |
| Gluteus Maximus | Posterior gluteal line of the ilium; posterior surface of the sacrum; side of coccyx; aponeurosis of sacrospinalis; sacrotuberous ligament; gluteal aponeurosis (fascia covering gluteus medius) | Superior fibers: the iliotibial tract of fasciae latae
Inferior fibers: gluteal tuberosity
|
Inferior gluteal nerve via L5, S1, S2 | Superior fibers: Hip extension, abduction, lateral rotation
Inferior fibers: hip extension Trunk extension when distal attachment of gluteus maximus is fixed (as in sitting to standing)
|
| Gluteus medius | External surface of ilium between the anterior and posterior gluteal lines | Lateral surface of greater trochanter of femur | Superior gluteal nerve via L5 and S1 | Abduction and medial rotation of femur |
| Gluteus minimus | External surface of ilium between anterior and inferior gluteal lines | Anterior surface of greater trochanter of femur | ||
| Tensor fasciae latae | Anterior superior iliac spine; anterior portion of iliac crest | Iliotibial tract | Tenses the fasciae latae and iliotibial tract; hip flexion, abduction, and medial rotation | |
Deep Layer
As their name “the lateral rotators” dictates, their primary action is lateral (external) rotation of the hip. In conjunction with the surrounding hip ligaments, the lateral rotators work to maintain hip-joint stability via increasing the congruency of the femoral head in the acetabulum. This role is much like that of the rotator cuff muscles in the upper limb that provide stability of humeral head within the glenoid fossa at the glenohumeral joint.
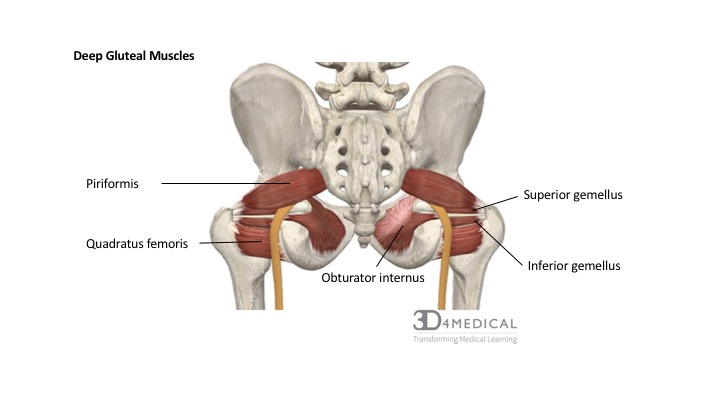
Figure 9. Diagram demonstrating the posterior view of the deep gluteal muscles.
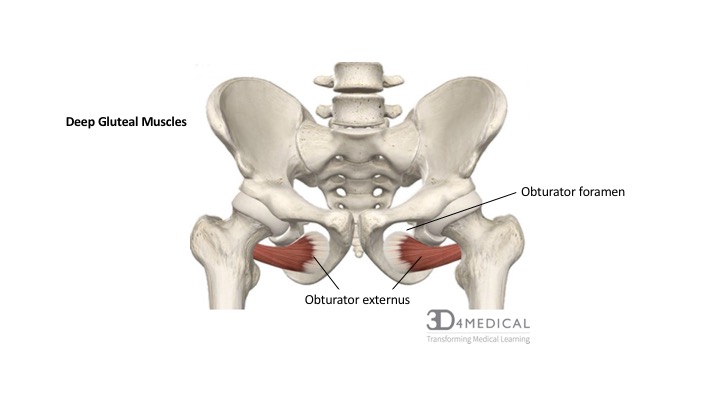
Figure 10. Diagram demonstrating the anterior view of the obtruator externus location on the pelvis to the femur.
Piriformis
Structure
Laying deep to the gluteus maximus is the piriformis, a flat, pear-shaped muscle originating on the anterior surface of the sacrum and spanning inferolaterally through the greater sciatic foramen towards its insertion point on the superior border of the greater trochanter of the femur.
The piriformis has been described as the landmark of the gluteal region given that blood vessels and nerves travelling to or through the pelvis are named for their position relative to it. As the piriformis exits the greater sciatic foramen, it divides the space into the suprapiriform foramen and the infrapiriform foramen. The superior gluteal artery and superior gluteal nerve exit the pelvis via the suprapiriform foramen while the inferior gluteal nerve, inferior gluteal artery, the sciatic nerve, the nerve to quadratus femoris, pudendal, and posterior femoral cutaneous nerve all exit via the infrapiriform foramen.
Given the vast amount of structures that pass inferiorly piriformis and considering that the piriformis itself almost completely fills the space of the greater sciatic foramen, the piriformis is often implicated in a common clinical condition of the gluteal region known as piriformis syndrome (see clinical conditions of the pelvis).
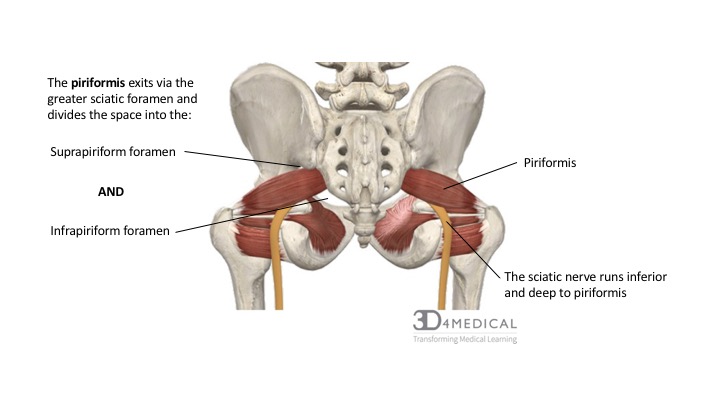
Figure 11. Diagram demonstrating the posterior view of the piriformis muscle orientation, origin and insertion on the pelvis and femur.
Function
The piriformis is responsible for lateral hip rotation, abduction when the hip is flexed, a small amount of hip extension, as well as for providing stabilization of the femoral head within the hip joint.
Innervation
The piriformis innervated by the nerve to piriformis, derived from the spinal nerves of S1 – S2.
Obturator Internus and Gemelli
Known as the triceps coxae or the triceps (three-headed muscle) of the hip, the obturator internus, superior gemellus and inferior gemellus all unite to fill the space between the piriformis and the most inferior lateral rotator, the quadratus femoris.
Structure
The obturator internus is a unique muscle in that it travels an extreme angular course to arrive at its insertion point on the greater trochanter. Originating on the inner surface of the obturator foramen, the obturator internus travels through the lesser sciatic foramen taking a right-angle turn, uniting with the distal tendinous insertions of both gemelli and all inserting into the trochanteric fossa of the femur.
The smaller and slender gemelli (superior and inferior) originate on the ischial spine and ischial tuberosity of the ischium, before travelling in a horizontal fashion to insert into the intertrochanteric crest of the femur along with the obturator internus.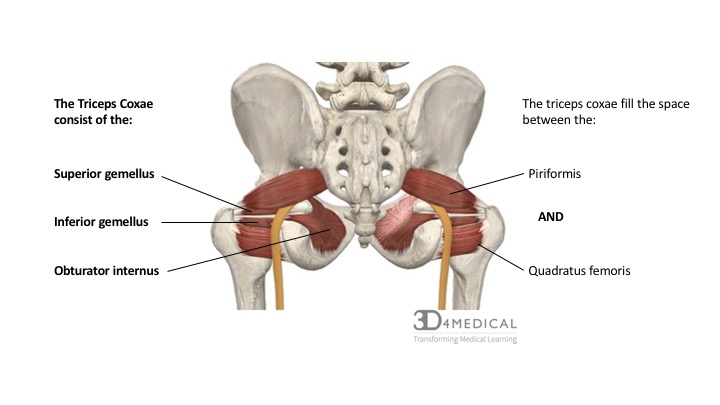
Figure 12. Diagram demonstrating the posterior view of the superior and inferior gemellus muscles origin and insertion on the pevlis and femur.
Function
The obturator and both gemelli (the triceps coxae) function synergistically to produce lateral hip rotation. These muscles can produce movement only when all three are functioning. Individually the obturator internus, superior gemelli and inferior gemelli are incapable of producing movement.
Innervation
Despite this shared insertion point and the close proximity of these muscles, the obturator internus and gemellus superior share a common innervation via the obturator nerve (L5 – S2), while the gemellus inferior is innervated via the nerve to the most inferior lateral rotator, the nerve to quadratus femoris (L4 – S1).
Obturator Externus
Structure
The obturator externus muscle is the most anteriorly situated on the pelvic girdle of all the deep lateral rotators. Because of its location, posterior to pectineus and the origins of the adductor muscles, it is often grouped with the adductor muscles.
Flat and fan-shaped, the obturator externus is a deep muscle originating from the external surface of the obturator membrane and margins of the obturator foramen, passing under the acetabulum and femoral neck to insert of the posterior aspect of the greater trochanter (trochanteric fossa).
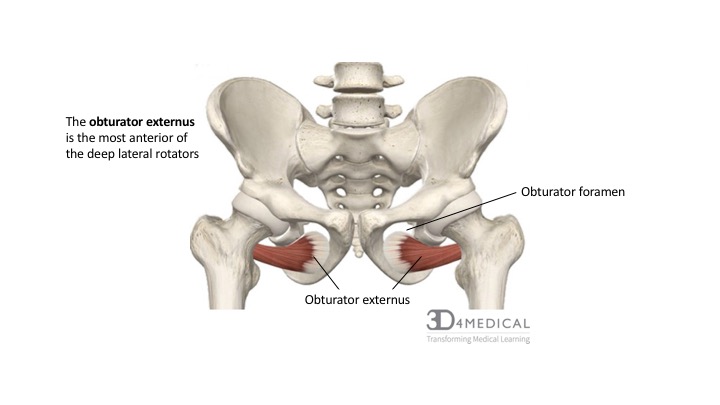
Figure 13. Diagram demonstrating the anterior view of obturator externus.
Function
The obturator externus is responsible for lateral (external) hip rotation and is activated primarily when the hip is flexed.
Innervation
Obturator externus is innervated via the obturator nerve (L3, L4).
Quadratus Femoris
Structure
As its name implies, the quadratus femoris is a stout rectangular muscle and is the most inferior of the deep lateral rotator musculature. Originating on the lateral border of the ischial tuberosity of the ischium, the quadratus femoris inserts onto the quadrate tuberosity of the femur.
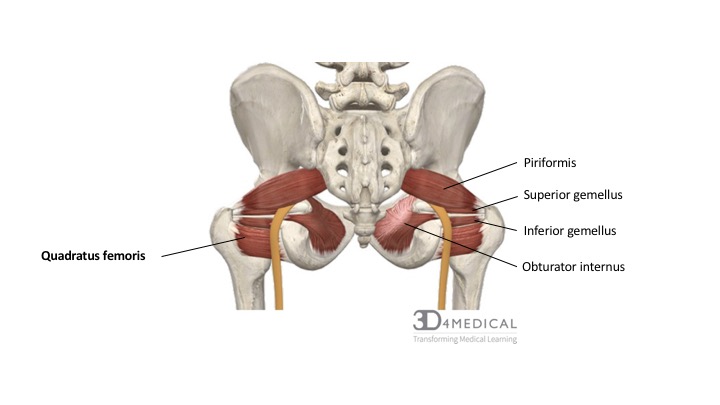
Figure 14. Diagram demonstrating the posterior view of the muscles in the lateral rotator group.
Function
The quadratus femoris is one of the stronger lateral hip rotators and also effectively functions to adduct the hip.
Innervation
The quadratus femoris is innervated via is own nerve, the nerve to quadratus femoris (L5 -S1).
| DEEP MUSCLES OF THE GLUTEAL REGION | ||||
| Muscle | Origin | Insertion | Innervation | Action |
| Piriformis | Anterior surface of the sacrum; sacrotuberous ligament | Superior border of greater trochanter of femur | S1 and S2 spinal nerves | Lateral hip rotation, abduction and extension; stabilization of femoral head in acetabulum |
| Obturator internus | Inner surface of obturator foramen and surrounding bones | Medial surface of greater trochanter of femur | Nerve to obturator internus via L5 and S1 | Laterally rotates the thigh when extended; abducts the thigh when flexed; stabilization of femoral head in acetabulum |
| Obturator externus | Outer surface of obturator foramen; superior ramus of pubis; inferior ramus of pubis; | Trochanteric fossa of the femur | Obturator nerve via L3 and L4 | |
| Superior gemellus | Ischial spine of ischium | Medial surface of greater trochanter with obturator internus | Nerve to obturator internus via L5 – S2 | |
| Inferior gemellus | Ischial tuberosity of ischium | Medial surface of the greater trochanter with obturator internus | Nerve to quadratus femoris
via L4 – S1 |
|
| Quadratus femoris | Lateral border of ischial tuberosity | Intertrochanteric crest of the femur | Nerve to quadratus femoris via L5 and S1 | Laterally rotates thigh; hip adduction; stabilization of femoral head in acetabulum |
The Pelvic Floor
Introduction
The pelvic floor creates a muscular wall within the bony structure of the pelvis, with hiatuses or openings through which the anus and urogenital organs penetrate. The coccygeus and the levator ani muscles make up most of the pelvic floor. The perineum is the diamond-shaped area located inferior to the pelvic floor. The anterior portion of the perineum is the urogenital triangle.
The pelvic floor has the five S‘s for main functions. Support – the pelvic floor is support for the urinary bladder, uterus (female), bowels, and some elements of the spine. Sphincteric – the pelvic floor muscles act as a continence mechanism to the urethral, anal and vaginal openings. Stability – because of their attachments to the pelvis, the pelvic floor muscles play an important role as part of the “core.” They assist other abdominal, pelvic, and spine muscles to control the movement of the sacroiliac and hip joints. Sexual – the pelvic floor muscles help achieve an erection and allow for penetration as well as play an important role in achieving orgasm. Sump-pump – the pelvic floor muscles help pump blood and lymphatic fluid back up towards the heart.
Muscles of the Pelvic Floor.
The video below depicts a cadaver dissection of the perineum and pelvic floor. The video is directly from the University of Wisconsin School of Medicine and Public Health.
https://viuvideos.viu.ca/media/09+The+Perineum/0_klcvmoco
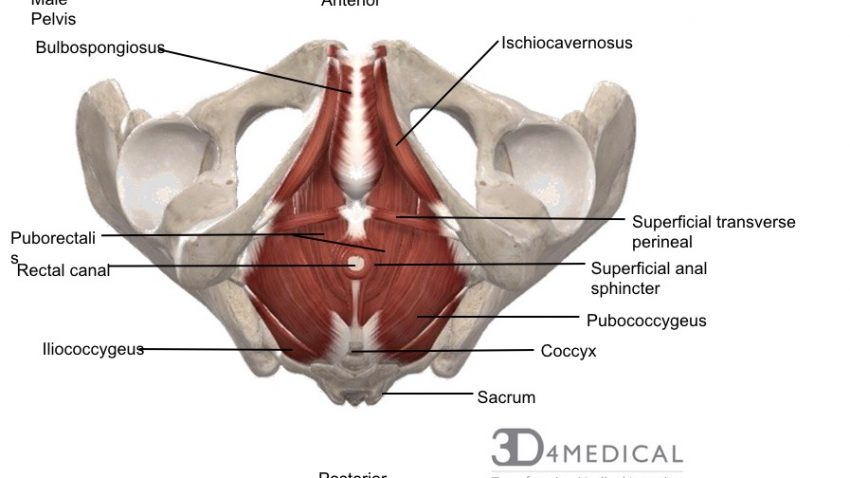
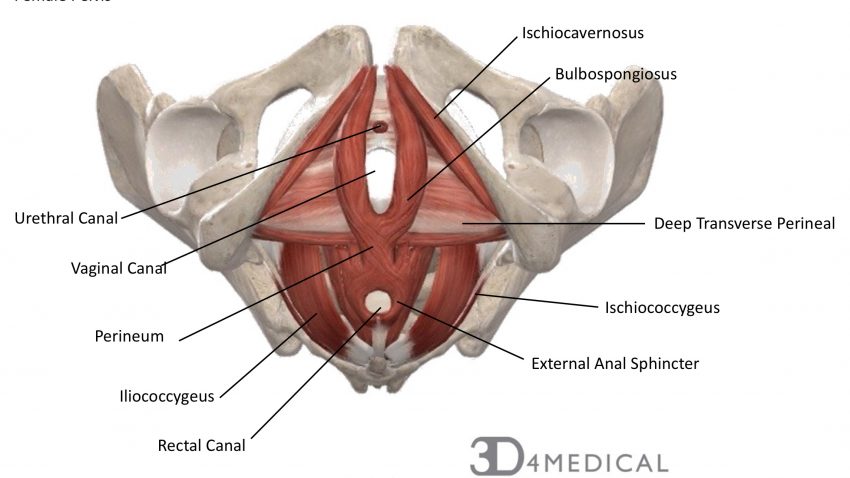
Layer One: Urogenital Triangle (Most Superficial): This layer is comprised of the bulbospongiosus, ischiocavernosus, superficial transverse perineal, and the external anal sphincter. This layer makes up the anterior portion of the perineum.
| Muscle | Origin | Insertion | Action | Innervation |
| Bulbospongiosus | Male: median raphe, ventral surface of bulb of penis
Female: perineal body then divides to wrap around vagina |
Male: Corpora spongiosum and cavernosa, fascia of bulb of penis
Female: fascia of corpus cavernosa
|
Male: Empties urethra, acts as sphincter to compress bulb of penis, assists erection, propels semen down urethra
Female: empties urethra, acts as a sphincter to reduce lumen of vagina and assists erection of clitoris
|
Deep branch of perineal
nerve (branch of pudendal nerve) |
| Ischiocavernosus | Ischial ramus and tuberosity | Crus of penis or clitoris | Maintains erection of penis or clitoris by compression of outflow veins | Deep branch of perineal nerve (branch of pudendal nerve) |
| Superficial transverse perineal | Ischial tuberosity | Perineal body | Reinforces action of deep transverse perineal muscle to stabilize perineal body | Deep branch of perineal nerve (branch of pudendal nerve) |
| External anal sphincter | Perineal body and encircles anal canal | Coccyx | Part of voluntary sphincter of anal canal | Inferior rectal (anal) nerve |
Layer Two: Urogenital Diaphragm (Deep to Urogenital Triangle): The urogenital diaphragm is a strong muscular membrane that sits between the symphysis pubis and ischial tuberosity. It stretches across the triangular anterior portion of the pelvic outlet. It is located inferior and superficial to the pelvic diaphragm.
Layer Three: Pelvic Diaphragm (Deep to Urogenital Diaphragm):
The pelvic diaphragm is a wide and thin muscular partition of tissue that forms the inferior border of the abdominopelvic cavity. It separates the pelvic cavity above from the perineal region below. The pelvic diaphragm is made up of the urethral sphincter (sphincter urethrae), deep transverse perineal, the perineal membrane and in females, compressor urethrae and sphincter urethral vaginalis. It is made up of a wide, funnel-shaped sling of fascia and muscle. It spreads from the symphysis pubis to the coccyx and across from one lateral sidewall to another. The pelvic diaphragm is supplied by the ventral rami of sacral nerve 3 & 4. It functions as a support system for the pelvic viscera, resists increases in abdominal pressure, and aids in micturnutation (passing of urine).
| Muscle | Origin | Insertion | Action | Innervation |
| Sphincter urethrae | Inferior aspect of pubic ramus and ischial tuberosity | Surrounds urethra; in females, some fibres also enclose the vagina | Controls flow of urine through urethra; also compresses vagina in females | Deep branch of perineal nerve (branch of pudendal nerve) |
| Compressor urethrae(only in females) | Ischiopubic ramus | Vaginal wall | Compresses ventral wall of the urethra | |
| Sphincter urethral vaginalis(only in females) | Vaginal walls | Ventral surface of urethra | Compresses ventral wall of the urethra | |
| Deep transverse perineal | Inner aspect of ischiopubic ramus | Median raphe (male), perineal body and external anal sphincter | Fixes perineal body, supports the function of levator ani and sphincter urethra | Deep branch of perineal nerve (branch of pudendal nerve) |
| Perineal membrane (fascial thickening, not a muscle) | Fasical attachments at pubic symphysis | Fascial attachments at ischial spine | Suspensory ligament that provides extra support to prevent descent of perineal body | |
Levator Ani Muscle Group
The levator ani muscle group consists of the puborectalis, iliococcygeus, coccygeus and in females only, pubovaginalis. The levator ani muscle group acts as support structures for urinary control and plays a vital role in supporting the pelvic organs. During childbirth or at an advanced age, damage or strength loss may occur with the levator ani muscle group, leading to urinary incontinence (refer to Pelvic Clinical Conditions section).
| Muscle | Origin | Insertion | Action | Innervation |
| Levator Ani Group | ||||
| Puborectalis | Dorsal surface of pubis and fascia of obturator internus | Unites with its partner to make a U-shaped sling around the rectum | Controls defecation by pulling anorectal junction forward | Nerve to levator ani (branches of S4), branch of pudendal nerve (S2-4) |
| Pubovaginalis | Nerve to levator ani (branches of S₄), branch of pudendal nerve (S₂-S₄) | |||
| Iliococcygeus | Posterior aspect of arcus tendineus levator ani and the ischial spine | Anococcygeal body and the coccyx | Helps to support pelvic viscera and lateral coccyx | Nerve to levator ani (branches of S4), inferior rectal nerve (from pudendal nerve – S3, S4), coccygeal plexus |
| Coccygeus | Ischial Spine | Lower two sacral and upper two coccygeal spinal segments, blends with sacrospinous ligament on its external surface | Supports pelvic viscera, flexion of coccyx, stabilizes sacro-iliac joint | Anterior rami of S4 and S5 |
Other Muscles of the Pelvic Floor
The obtruator internus muscle lines most of the lateral wall of the pelvis (refer to gluteal region). The piriformis muscle covers most of the posterior wall of the pelvis (refer to gluteal region).
The video above depicts the muscles of the pelvic floor. It can be found at: https://www.youtube.com/watch?time_continue=165&v=P3BBAMWm2Eo
