Lower Limb
The Foot
The foot is an incredibly complex mechanism. Each foot contains 26 bones, 33 joints, and more than a hundred muscles, tendons, and ligaments. These parts work harmoniously to get you from one place to the next. They do it all while handling hundreds of tons of force – your weight in motion – every single day. They are truly amazing structures, however, the stress of carrying you around creates a lot of wear in tear which, in turn, puts your feet at a higher risk of injury than any other part of your body. In this section, we will discuss the muscles, bones, ligaments, tendons and clinical conditions of the foot.
Muscles of the Foot
The muscles acting on the foot can be divided into two distinct groups; extrinsic and intrinsic muscles.
- The extrinsic muscles arise from the anterior, lateral, and posterior compartments of the leg. They are mainly responsible for actions such as eversion, inversion, plantarflexion, and dorsiflexion of the foot.
- The intrinsic muscles are located within the foot and are responsible for the fine motor actions of the foot, for example, movement of individual digits.
Extrinsic Muscles
In terms of anterior leg muscles that insert onto the foot, there is a helpful mnemonic to remember the order and names of them. Tom, Dick And Nervous Harry stands for tibialis posterior, flexor digitorum longus, tibial artery, tibial nerve, and flexor hallucis longus. These five tendons and nerves all run down in order from closest to the medial malleolus to furthest, underneath the medial malleolus on their way to their attachment point (see figure 1).
Tom, Dick And Nervous Harry
- Tibialis Posterior
- Flexor Digitorum Longus
- Posterior Tibial Artery
- Tibial Nerve
- Flexor Hallucis Longus
The posterior leg muscles that insert on the foot are the: gastrocnemius, plantaris, soleus, tibialis posterior, flexor digitorum longus, and flexor hallucis longus. Collectively, the posterior leg muscles work to plantarflex and invert the foot. They are innervated by the tibial nerve.
The lateral leg muscles that insert on the foot are the fibularis longus and fibularis brevis. These two muscles perform eversion of the foot and are innervated by the superficial fibular nerve.
Intrinsic Muscles
The intrinsic muscles of the foot can be further broken down into the dorsal aspect and the plantar aspect.
- Dorsal Aspect – there are only two intrinsic muscles located in the dorsum of the foot, however many of the extrinsic muscles discussed previously attach here. The two muscles found in this area are the extensor digitorum brevis and the extensor hallucis brevis. These muscles are mainly responsible for assisting some of the extrinsic muscles in their actions. Both muscles are innervated by the deep fibular nerve.
- Plantar Aspect – There are four plantar layers of the foot, containing ten intrinsic muscles. The muscles act collectively to stabilize the arches of the foot, and individually to control movement of the digits. Below are the four plantar layers of the foot. If the layer heading has an ‘A’ in it, there are no muscles present in this layer. If it does not have an ‘A’, this layer contains muscles. For example, ‘Layer 1A’ is a non-muscular layer, as it is only comprised of the plantar aponeurosis.
Layer 1A
- Plantar Aponeurosis
Layer 1
- Flexor Digitorum Brevis
- Abductor Hallucis Brevis
- Abductor Digiti Minimi
Layer 2A
- Tendon Flexor Hallucis Longus
- Tendon Flexor Digitorum Longus
Layer 2
- Lumbricles
- Quadratus Plantae
Layer 3
- Flexor Digiti Minimi
- Adductor Hallucis Brevis
- Flexor Hallucis Brevis
Layer 3A
- Long Plantar Ligament
- Tibialis Posterior
- Fibularis Longus
Layer 4
- Plantar Interosseus
- Dorsal Interosseus
Bones of the Foot
The bones of the foot help the foot withstand weight from the body while standing as well as in motion. They can be divided into three groups (see figure 2):
- Tarsals – a set of seven irregularly shaped bones. They are situated proximally in the foot in the ankle area.
- Metatarsals – connect the phalanges to the tarsals. There are five in number – one for each digit.
Phalanges – the bones of the toes. Each toe has three phalanges – proximal, intermediate and distal (except the big toe, which only has two phalanges).

Figure 2 Three bone groupings of the foot. Retrieved from https://teachmeanatomy.info/lower-limb/bones/bones-of-the-foot-tarsals-metatarsals-and-phalanges/
Furthermore, the tarsal group can be divided into three more groups: the proximal tarsals, intermediate tarsals, and distal tarsals. The proximal tarsal bones are comprised of the talus and calcaneus. These bones form the bony framework around the proximal heel and ankle joint. The intermediate row of tarsal bones contains one bone, the navicular (given its name because it is shaped like a boat). Finally, the distal tarsals contain four tarsal bones, the most bones out of the tarsal subgroups. It contains the cuboid, as wells as the lateral, intermediate, and medial cuneiform bones. There is a simple mnemonic to remember all of the tarsal bones and their position relative to each other. It is: Tiger Cubs Need MILC.
Moving clockwise around the foot, the ‘T’ in Tiger represents the talus, which is the most proximal, medial tarsal bone. The ‘C’ in Cubs represents the calcaneus, which is the most proximal lateral tarsal bone. The ‘N’ in Need represents the navicular, which is distal to the talus and lateral to the cuboid. Continuing to move clockwise, we reach the cuneiform bones, which are represented by the ‘M’, ‘I’, and ‘L’, in MILC. The ‘M’ represents the medial cuneiform, the ‘I’ represents the intermediate cuneiform, and the ‘L’ represents the lateral cuneiform. Lastly, the ‘C’ in MILC represents the cuboid, which is lateral to the cuneiforms and distal to the calcaneus. That covers all the tarsal bones, and remembering the mnemonic is a simple way to remember the position of the bones of the foot starting proximally and moving clockwise.
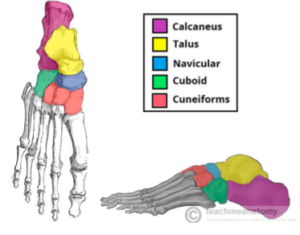
Figure 3 The tarsal bones of the foot. Retrieved from https://teachmeanatomy.info/lower-limb/bones/bones-of-the-foot-tarsals-metatarsals-and-phalanges/
Continuing to move distally, we reach the metatarsals of the foot, which are proximal to the phalanges but distal to the tarsals. There are five metatarsals that are numbered I-V, medially to laterally. They all have similar shape and structure.
After the metatarsals, we reach the phalanges. The phalanges are the bones of the toes and consist of proximal, middle, and distal bones. The only toe that doesn’t have these three phalanges is the big toe, which only has proximal and distal phalanges (see figure 3).
The bones of the foot are very important for several aspects of life, and many clinical conditions can arise from injuries or conditions that may be present in this area. Continue reading to learn some of the clinical conditions associated with the foot.
Joints of the Foot
- Subtalar Joint
- Transverse Tarsal Joint
- Metatarsal Joint
- Interphalangeal Joint
Subtalar Joint– This is named because of the location of the meeting point of the talus and the calcaneus. The talus connects with the calcaneus just beneath it. Hence the term “Subtalar”. This joint is important because it allows for inversion and eversion of the foot.
Transverse tarsal joint– The transverse tarsal joint is a complex joint seeing as it consists of both the Calcaneocuboid joint and the talonavicular joint. This joint creates most of the ability of supination and pronation of the foot.
Metatarsal Phalangeal Joint, also known as the metatarsophalangeal joint. There are five metatarsal-phalangeal joints and they are all where the metatarsal of the foot connects with their matching proximal phalanges.
Interphalangeal joint, include all of the joints that connect the phalanges (toes) together. All Phalanges except for the hallux have two interphalangeal joints; the proximal interphalangeal joint, and the distal phalangeal joint. The hallux only contains one joint, and that’s the interphalangeal joint.
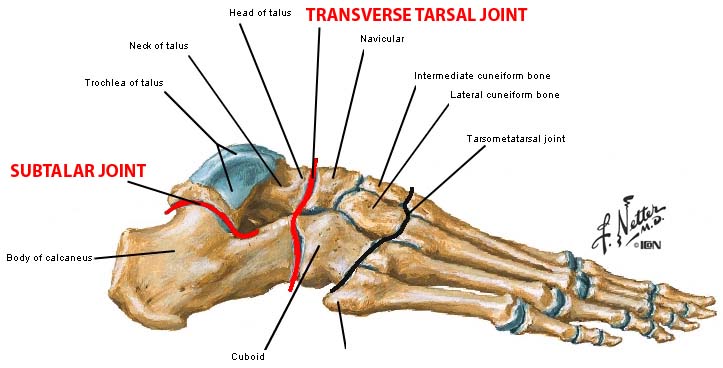
Retrieved from http://anatomybody101.com/bones-and-joints-of-the-foot/bones-and-joints-of-the-foot-transverse-tarsal-joint/
Ligaments of the Foot
There are over 30 ligaments in the foot. They connect bones to other bones to form joints. There are three main ligaments of the foot:
- plantar fascia – the longest ligament of the foot. The ligament, which runs along the sole of the foot, from the calcaneus to the phalanges, forms the arch of the foot. By stretching and contracting, the plantar fascia helps us balance and gives the foot strength for walking.
- plantar calcaneonavicular ligament– (Commonly known as the plantar ligament) it is a ligament of the sole of the foot that connects the calcaneus and navicular and supports the head of the talus. This ligament lays deep to all the other ligaments.
- calcaneocuboid ligament–the following ligament connects the calcaneus and the tarsal bones and helps the plantar fascia support the arch of the foot
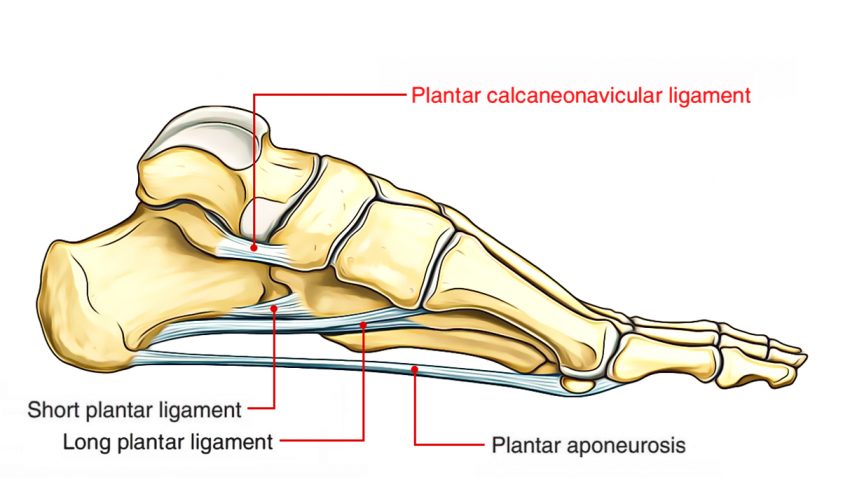
- Retrieved from https://www.earthslab.com/anatomy/plantar-calcaneonavicular-ligament/
Tendons of the Foot
There are several tendons of the foot, however the most notable is the Achilles tendon. The gastrocnemius and soleus unite into one band of tissue, which becomes the Achilles tendon at the distal end of the tibia. The Achilles tendon then inserts on the calcaneus. The Achilles tendon makes it possible to run, jump, climb stairs, and stand on your toes.
Retinaculum of the Foot
- Superior Extensor Retinaculum
- Inferior Extensor Retinaculum
- Flexor Retinaculum of the Foot
- Peroneal Retinacula (Superior and Inferior)
The retinacula are strong, fibrous, connective tissue bands that hold different tendinous groups together. These are primarily located in the hand/wrist and in the foot/ankle. These retinacula are located depending on which tendons they are meant to hold down along the foot. The superior extensor retinaculum is the superior section of this two-part retinaculum, used to constrain extensor digitorum longus, extensor hallucis longus, and tibialis anterior. The inferior extensor retinaculum has a similar purpose and is used for the same tendons as its counterpart but located slightly inferior to cover more surface area of the top of the foot. The flexor retinaculum of the foot is located on the medial side of the foot and is used to hold the Tom, Dick and Nervous Harry group together.
Clinical Conditions of the Foot
- Pigeon toe
- Hammer toe
- Plantar Fasciitis
- Jones Fracture
- Turf Toe
- Flat Foot
- Pes Cavus
- Cavovarus foot
Pigeon Toe
Description:
Otherwise known as in-toeing is a condition which causes the toes to point inward when walking. It occurs due to a femoral anteversion/torsion is the most frequent cause of in-toeing in children between the ages of 3-10 years. The femur is the long bone that goes from the hip to the knee. This angle is normally up to 15°, and an increased angle indicates pigeon toe.
Symptoms:
Symptoms are typically visible at birth:
- One or both feet will be turned inward
- Curved outer edge of foot, in a crescent shape
- Internal tibial torsion becomes obvious when infants start walking
Causes:
In man cases, pigeon toe develops in the womb, due to limited space some babies will grow in a way that forces their feet inwards. In other cases it develops as kids grow in their toddler years as begin to walk, it is characterized by internal tibial torsion which is a twisting of the tibia. Medial torsion more common in children three and older is when the femur beings to rotate inwards, girls are at a higher risk to develop medial torsion.
Treatment Surgical interventions:
The only specified treatment for general cases of pigeon toe consists of finding correct footwear and orthotics to increase comfort level and stability.
Hammer Toe
Description:
A hammer toe is a physical deformity of the proximal interphalangeal joint within the second, third, or fourth toe. This causes the joint to remain bent, giving the toe a claw-like appearance. Several genetic factors are known to place an individual at risk for developing hammertoe, including Morton foot. Hammertoe can also be caused by frequently wearing high-heeled, narrow, or ill-fitting shoes.
Symptoms:
A hammer toe will cause discomfort while walking, it will also cause pain when you try to extend the toe. Some other symptoms are as follows:
- Toe that bend downwards
- Calluses
- Difficulty walking
- Inability to flex your foot or wiggle your toes
- Claw-like toes
Causes:
An imbalance in the muscles surrounding the middle toe joint. These muscles, tendons, and ligaments work together to bend and straighten the toes. If one of the muscles weakens, it cannot bend or straighten the toe. If the toe stays bent long enough, the muscles tighten and the toe will not be able to straighten out. Your two contains two joints, when your middle joint becomes flexed or bent downward for extended periods of time this can place you at risk for developing hammer toe.
Treatment & Surgical conditions:
Non-invasive treatments such as toe wraps, splints, toe pads, and gel toe pads can extensively improve the comfort of hammer toe and can decrease the likelihood of having surgery.Surgical interventions such as joint resection are the most common procedure where an incision is made over the top of the toe. Ligaments and tendons may also be cut to straighten the foot.
Plantar Fasciitis (PLAN-tur fas-e-I-tis)
Description:
Plantar Fasciitis is the pain in the heel or the back arch of your foot. The pain is coming from here because of the origin of the plantar fascia being at the tuberosity of the calcaneus. Plantar fasciitis pain comes when the plantar fascia becomes overstretched and results in a tear in the heel end of the ligament.
Symptoms:
Plantar fasciitis is characterized by a sharp stabbing pain in the bottom of the foot near the heel. The pain worsens by bearing weight after long periods of rest. Individuals with plantar fasciitis often report their symptoms are most intense during their first steps after getting out of bed or after long periods of sitting.
- Stabbing pain in the bottom of your foot near the heel
- Pain is typically at its worst in the first few steps
- Pain in the heel directly after exercise, but not always obvious during
Causes:
This can be caused because of sudden excessive running or walking, or the use of inappropriate footwear. Staying off of your feet and icing as much as possible, as well as constant stretching of your legs can treat Plantar Fasciitis. Among a population of runners, 4-22% of the population. Rano et al found that the average age of the patients presenting to their facility with heel pain was almost 10 years higher than controls who presented for other reasons
Treatment & Surgical conditions:
Treatments can be as simple as trying simple stretches and exercises to strengthen the foot and by wearing sturdy lace-up shoes. A more aggressive treatment suggested could be anti-inflammatory drugs, wearing a splint, cortisone injections or a costly surgery. The most common complications with a plantar fasciotomy derive from instability with lateral column pain and instability being most pronounced. When patients undergo a plantar fasciotomy, they lose some degree of support to the foot. This loss of support is usually temporary while the other structures adapt and accommodate to this loss.
Jones Fracture
Description:
The Jones fracture is an avulsion fracture at the base of the fifth metatarsal. The insertion of the Peroneal Brevis muscle is located on the base of the fifth metatarsal and with overuse and repetitive stress and trauma; the Peroneal Brevis will rip off the base of the fifth metatarsal.
Symptoms:
A Jones fracture has many of the same symptoms as other types of fractures. A person with a Jones fracture may know they have injured their foot right away if the injury is sudden and causes immediate symptoms.
- pain and swelling on the outside of the foot at the base of the little toe
- problems walking
- bruises
Causes:
This type of fracture typically results from stress on the bone caused by repeated motion, but it may also result from overuse or sudden acute injury.
Treatment & Surgical conditions:
In some cases surgery may be needed, but if not the RICE method (Rest, Ice, Compression, Elevation) is the best way to treat this condition. Since there is limited blood flow to the area, a Jones fracture has a higher chance of not healing than other metatarsal fractures, unless a person has surgical treatment.
Complications of surgery include:
- problems related to surgery and anesthesia, such as blood clots
- the need for repeated surgery
- refracturing after healing
- muscle atrophy
- continued pain and swelling
- Turf Toe
Description:
Turf toe is the common term used to describe a sprain of the ligaments around the big toe joint. These ligaments work to primarily as a hinge to permit up and down motion. The hyperextension of the big toe repeatedly over time with enough force can cause the sprain in the ligaments that surround the joint.
Symptoms:
Symptoms typically develop slowly, and worsen over time
- Pain, swelling, and limited movement of the joint at the base of the big toe
- In some cases a pop can be felt
Cause:
The main cause of this is by athletes jamming their toe into the hard ground (turf) repetitively. Usually happens in the sport of soccer and football.Turf toe is a sprain due to hyperextension of the hallux at the metatarsal phalangeal joint.
Treatment & Surgical interventions:
The best way to treat turf toe is the RICE method (Rest, Ice, Compression, Elevation).
Flat Foot
Description:
Otherwise known as Pes Planus, is the condition where there is little to no medial longitudinal arch. Estimated 20-30% of the population has some degree of Pes Planus. People with flat feet may roll to the inner side of where they are standing and walking. Anatomically known as overpronation, and it also causes the foot to point outward.
Symptoms:
In some cases there will be no obvious symptoms of flat foot. Some include:
- Pain on the inside of the arch, or pain radiating along the outside of the foot below the calcaneus
- Generalized foot fatigue
Causes:
Arises from the foot losing its normal structural support, thus altering shape. An imbalance in the forces that tend to flatten the arch and those that support the arch can lead to loss of the medial longitudinal arch. Due to flat feet, there are abnormal stresses on the knee and hip that results in pain in the joints. These stresses are likely if the ankle turns inward. Pain most commonly affects the following parts of the body: Arch of the foot, calf, knee, hip, lower back and lower leg. The pain is caused by an uneven distribution of the body weight.
Treatment & Surgical interventions:
Treatment for flat feet depends on the severity. If flat feet cause no pain or other difficulties, then treatment is probably not needed. Treatment for pain inducing flat foot could be as follows; Stretching exercises, physical therapy, occupational therapy and pain medication could aid in the relief of pain and foot damage. If surgery is recommended, there could be several options of what he treatment will consist of. Such as, fusing foot or ankle joints together, removing bones, cleaning the tendons protective layers and more.
The following video is a surgical video, viewers may find the content disturbing.
https://youtu.be/TkTdN4NxNZM
The following video is a surgical video, viewers may find the content disturbing.
Pes Cavus (pes ca· vus)
Description:
Also known as Cavus Foot, Pes Cavus is the condition of a high medial longitudinal arch. You can inherit it, get it through trauma, or get it through neuromuscular conditions. Pes Cavus can be very bad for your feet, but fortunately, it can be treated. The best treatment for this are orthopedics and shoe modifications.
Symptoms:
If properly cared for they are asymptomatic. Due to the pressure among the metatarsals if the arches aren’t flexible some people will experience the following symptoms:
- Foot pain leading to significant decrease in foot function
- Metatarsalgia, pain under the first metatarsal
- Plantar fascitis
- Achilles tendonitis
Causes:
Pes cavus may be hereditary or acquired, the underlying causes are commonly neurological, orthopaedic, or neuromuscular. Some factors that contribute to pes cavus may include weakness and imbalance in neuromuscular disease, and residual effects of congenital clubfoot.
Treatment & Surgical Interventions:
Non-surgical rehabilitation approaches include, stretching and strengthening of tight and weak muscles, massage, chiropractic manipulation, and strategies to improve balance. There are a few surgical procedures that are considered in extreme cases. First, soft-tissue procedures (e.g. plantar fascia release, Achilles tendon lengthening, tendon transfer); second, osteotomy (e.g. metatarsal, midfoot or calcaneal); lastly, bone-stabilising procedures (e.g. triple arthrodesis).
Cavovarus Foot (cav-O-var-us)
Description:
Cavus (elevated Longitudinal Arch) of the 1st ray and forefoot pronation and Varus is hind foot. Cavovarus foot deformity, which often results from an imbalance of muscle forces is commonly caused by hereditary motor sensory neuropathies. It is seen in both Pediatric and adult populations with 67 percent due to a neurological condition.
Symptoms:
- Hammer toes, or claw toes
- Calluses on the ball, or heel of the foot
- Pain when stationary, or when partaking in physical activity
- Unstable feet due to the heel tilting inward, which in some cases puts individuals at risk for ankle sprain
Causes:
Neurological conditions diagnosis is critical to render appropriate treatment. Bilateral condition is most commonly Charcot-Marie tooth disease (CMT) The muscle imbalances generate deformity in a weak tibialis anterior and peroneus brevis overpowered by strong peroneus longus and posterior tibialis which results in plantar flexion 1st ray and forefoot pronation with compensatory hindfoot varus.
Treatment & Surgical interventions:
Treatment on a lower scale of severity could only require physiotherapy or occupational therapy. In more severe cases, several surgical approaches would be necessary such as Soft-tissue surgery, tendon transfers, bone surgery and calcaneal osteotomy. Some complications can arise such as; ankle instability, standard lateral ankle ligament reconstruction will fail if cavovarus deformity is not concomitantly addressed. If cavovarus is untreated can lead to varus ankle arthritis.
The following video is a surgical video, viewers may find the content disturbing.
The following video is a surgical video, viewers may find the content disturbing.
